The institutional review board of Aix Marseille University, Marseille, France approved the therapeutic assay, and both patients included in this study gave her consent for non-conventional treatment as well as for the clinical report. For establishing the pump device, we used the teriparatide pre-filled pen (teriparatide; European Union trade name, Forsteo; U.S. tradename, Forteo; 20µg/80µl,1ml = 250µg of teriparatide; Lilly France) and the Omnipod® pump (Insulet Corp., Boston, MA) in which two milliters represent a total of 200 international units (IU). Omnipod is usually employed for insulin administration [19]. We diluted 1.2 ml of teriparatide to 0.8 ml of sterile water for injection, as previously described [20] to reach a total volume of 2 ml in the reservoir of the pump. As such, 200 IU in the pump equal to 300 µg of teriparatide. The reservoir and the infusion sets were changed every 3 days by a qualified nurse in a first time, then by the patients.
We initiated a flow of 0.5 IU/hour, which corresponding to 18 µg/24h of rhPTH (1-34), an initial dose close to the one reported to be effective in other case reports [21–23]. During hospitalization stay, we daily adapted the flow depending on the calcemia of the patient. After hospital discharge, the flow was adapted on the protocol we established, to reach corrected calcemia level between 2.15 and 2.40 mmol/L (Figure 1).
Practically, the patient was hospitalized the day before we initiated the pump infusion, for a complete laboratory workup and an electrocardiogram. On day 2, we started the pump (6.00am), and calcitriol (1µg) was given to the patient in the morning (6.00 am) and the afternoon (6.00 pm), after what, all the oral medications were discontinued. The patient was hospitalized for a theoretical stay of seven days, which could have been longer if necessary.
Vital clinical parameters were daily recorded. The biochemical analysis at admission included albuminemia, total/corrected calcemia, phosphatemia, magnesemia, 25OH vitamin D, serum creatinine and urinary calcium excretion (UCR, appreciated by the ratio mmol calcium/mmol creatinine. Albuminemia, total/corrected calcemia, phosphatemia and UCR were daily assessed during hospitalization. After hospital discharge, total/corrected calcemia and phosphatemia were weekly assessed. Every month, 25OH vitamin D level and UCR were measured. In case of hypo-/hypercalcemia and/or modification of the pump flow, total/corrected calcemia was systematically analyzed after 24 hours.
Assays
Calcemia was measured by automated techniques, with a normal range of 2.2 - 2.55 mmol/L and adjusted for albumin by the following formula: Corrected calcemia = 0.025 x (40 - albuminemia). Phosphatemia, magnesemia and creatinine were also measured by automated techniques. Urinary calcium was measured by colorimetric method.
Clinical Cases
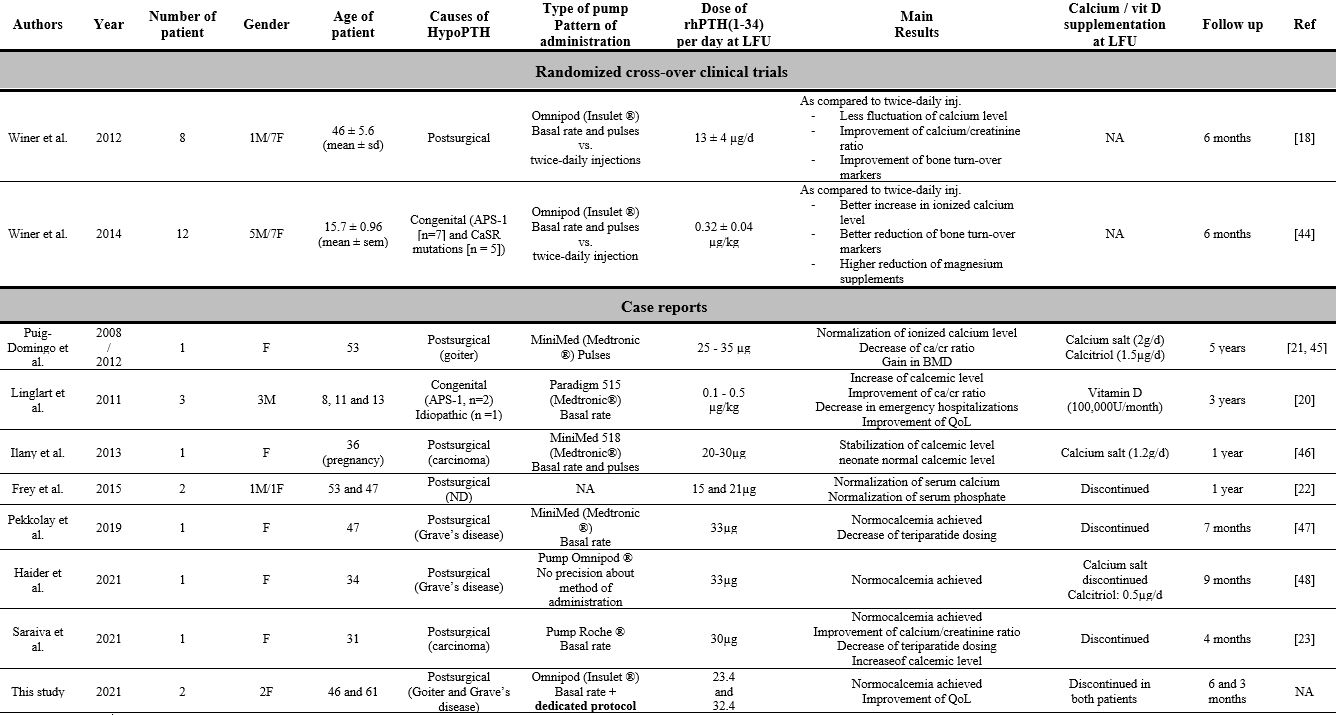
Patient 1 is a woman born in 1975 and referred to our center in 2016 for the treatment of a chronic hypoPTH. She underwent a total thyroidectomy in 2015 for a benign multinodular goiter. HypoPTH occurred in the immediate postoperative period. We first met her in 2017, after she was referred by her surgeon to our department (the patient was aged 42). She had no medical history of kidney stones or evidence of it on specific imaging (kidney ultrasonography and CT scan). Bone mineral density (BMD) assessed by X-ray absorptiometry (DXA) remained stable between 2018 and 2021 with a T-score (bone lumbar and hip) in the normal range (-0.2 and 0.1 SD, respectively). Circulating PTH was undetectable, always below 4 pg/mL (N: 10 - 65 pg/ml) and calcemia always remained below 2 mmol/L, while she was treated with high doses of calcitriol (Rocaltrol®, 3µg x 3/d) and oral calcium carbonate (2g x 4/d) (Table 1). Investigations ruled out poor therapeutic compliance and/or digestive malabsorption. Urinary calcium was high, comprised between 4.8 and 7.2 mg/kg/24h (Upper limit of normal: 4 mg/kg/24h), with an UCR of 1.3 (N < 0.5). 25-hydroxyvitamin D level was at the lower limit of normal (61 nmol/L, N: 75-250). Magnesemia was in the normal range. At the clinical level, she complained of severe and disabled weakness, muscle cramps and joint pains, which not allowed her to practice her job. She was hospitalized at least once every three months for intravenous infusions of calcium gluconate for symptomatic hypocalcemia. Because PTH 1-84 is not available in our country, we started off-label twice-daily subcutaneous administration of rhPTH 1–34 at a dose of 20 µg/12h, according to previously published data [24, 25]. Her calcemia normalized and a significant improvement of her symptoms occurred for one month, after what, she experienced, again, symptomatic hypocalcemia despite 4 injections/d. Finally, we offered her to be treated with continuous teriparatide infusion using the Omnipod device system. At that time, she was aged 46 yo. Her calcemia normalized in the first 8 hours following the beginning of the infusion (Figure 3A) and a remarkable improvement of her clinical symptoms occurred in the first 48 hours. It is noteworthy that the patient stopped her antidepressive treatment with success. Her calcemia remained above 2 mmol/L until now (6 months up to now), except from week 14 to 20, where several episodes of hypocalcemia reoccurred. The later was related to a lipodystrophy in the site of injection of the pump catheter and has been resolved by changing the site of injection. Her UCR decreased from 1.18 To 0.37 after 6 months. Vitamin D supplementation was initiated (vitamin D3 100,000 IU every 3 months) and she succeeded to discontinue calcitriol and calcium supplementations.
Ultimately, the patient followed an educational program before hospital discharge that currently allows her to manage by herself the flow of the pump and filling its reservoir. On the last follow up, the flow of the pump was 0.65 UI/h corresponding to 23.4 µg of teriparatide per day. We plan to continue the treatment as long as her calcemia is normalized and her symptoms remains controlled. She will be followed every 6 months at the clinical levels and dedicating imaging procedures (radiography, MRI) will be performed if bone pain manifest.
Patient 2 is a 61 yo woman who was operated of total thyroidectomy in 2003 for Grave’s disease. She immediately developed hypocalcemia in the postoperative period with low levels of PTH. During 15 years she was treated with high dose of calcitriol (Rocaltrol®, up to 4x1µg thrice daily) and calcium carbonate (500mg) for a total of 5 g/d (Table 1). She was referred to our department for the first time in 2017. Because of the existence of Grave’s disease, we ruled out celiac or Biermer’s disease that could be the source of digestive malabsorption. Despite high doses of calcium and calcitriol, she experienced chronic asthenia, paresthesia of extremities, which not allowed her to exert any physical activities. In parallel, her calcemia remained below 1.8 mmol/L, the reason why she was regularly admitted in our unit for i.v. calcium gluconate treatment. Her magnesemia was normal and vitamin D level was low, at 45 nmol/l. Subcutaneous injection of teriparatide (20µg each, 3-times daily) were started in 2018, however were inefficient and calcemia level remained below 2 mmol/L. She was operated of a bilateral posterior subcapsular cataracts, a likely complication of her chronic hypoPTH, but no history of kidney lithiasis was recorded, or demonstrated by kidney imaging. Her BMD assessed by X-ray absorptiometry (DXA) showed osteopenia at the L1-L4 lumbar spine (Tscore -1.3 SD) and femoral neck (Tscore -1.7SD) levels.
In 2021, the patient gave her informed consent to be treated with continuous teriparatide infusion by the Omnipod device system. We started at 0.5UI/h and, eventually, reached a current flow of 0.9 UI/h. Once the pump was started, corrected calcemia reached after 16 hours, and for the first time, 2 mmol/L, then normalized from day 3. The patient noticed a very significant improvement in her clinical symptoms, more specifically, her joint and muscle pains fully disappeared. We did not observe any substantial change in her UCR. During the follow up, she needed continuous paramedical home care the first month to adapt the flow of the pump and to fill the reservoir. Because she had been operated of bilateral cataract, we paid attention that she could manage to fill the reservoir by herself. After 3 months, she is autonomous and the flow of the pump is 0.9UI/h (equivalent to 32.4 µg/d of teriparatide). Last but not least, she stopped her calcium and calcitriol supplementation, but we prescribed her vitamin D3 (100,000 IU every 3 months) because of her vitamin D deficiency. The treatment will be continued as long as it results in normalization of her calcemia and improvement of her quality-of-life. However, like for the other patient, a careful follow-up is planned twice-yearly at the bone level (physical exam and radiology in case of pain or palpated mass).
{kind=link}