Two hundred and eighty (280) completed surveys were returned, a 41% response rate. In terms of the interviews, although data saturation was reached after ten interviews, five more were conducted (n=15).
Demographics
Most participants were female (n=220; 89.8%), professional nurses (n=120; 51.3%) with a 4-year diploma in nursing (n=113; 48.3%) and permanently employed (n=236; 94.4%). The largest proportion of respondents were aged 35-45 years (n=98; 43.2%) and had 5-9 years of working experience in the current hospital (n=124; 59.6%).
Descriptive statistics
Table 2 presents responses for individual items and subscales.
Causes of medication error related to communication, human, environmental and medication-related factors were considered to have a moderate risk, with the following causes being the most common: high patient-to-nurse-ratio (M=3.44; SD 0.87), work overload (M=3.39; SD 0.89), inadequate staffing (M=3.36; SD 0.89), stock distribution problems (M=3.18; SD 0.96), high acuity level of patients (M=3.09; SD 1.0) and illegible prescriptions (M=3.05; SD 1.09). The three main causes of medication error were thus summarised as workload (including high patient-to-nurse ratio, work overload, inadequate staffing and patient acuity), stock distribution problems, and illegible prescriptions.
Most participants perceived medication errors as never occurring (n=60; 23.2%), or occurring a few times a year or less in their units (n=124; 47.9%). Only four respondents (1.5%) perceived that medication errors could occur in their units every day.
The majority of respondents perceived the overall grade of patient safety as excellent or very good (n=161; 61.5%).
Three safety culture items related to staffing shortages triggered concern: 83% (n=230) of respondents disagreed that there are enough staff to handle the workload, 72.3% (n=190) agreed that they work in “crisis mode”, doing too much, too quickly, and 70.5% (n=186) agreed that staff work longer hours than is best for patient care. However, on the positive side, nurses felt that they are actively attempting to improve medication safety (n=239; 90.5%), that people support one another in the unit (n=216; 80%), and that their procedures and systems are good at preventing errors (n=210; 80.2%).
Most degrees of error severity were only reported sometimes, although the errors that could cause harm to the patient were reported more often, albeit not always. A quarter of participants (n=60; 26%) perceived that medication errors that cause harm to patients were never or rarely reported, while 32.9% (n=77) perceived that errors that could potentially harm the patient were never or rarely reported.
The main reasons for not reporting medication errors were fear and administrative response, where the following items were rated highest: nurses are blamed if something happens to patients (M = 4.47; SD 1.84), individuals rather than systems are implicated for errors (M= 4.10; SD = 1.93), and the patient or family may develop a negative attitude toward the nurse (M=4.05; SD 2.02).
Correlations between individual items and subscales
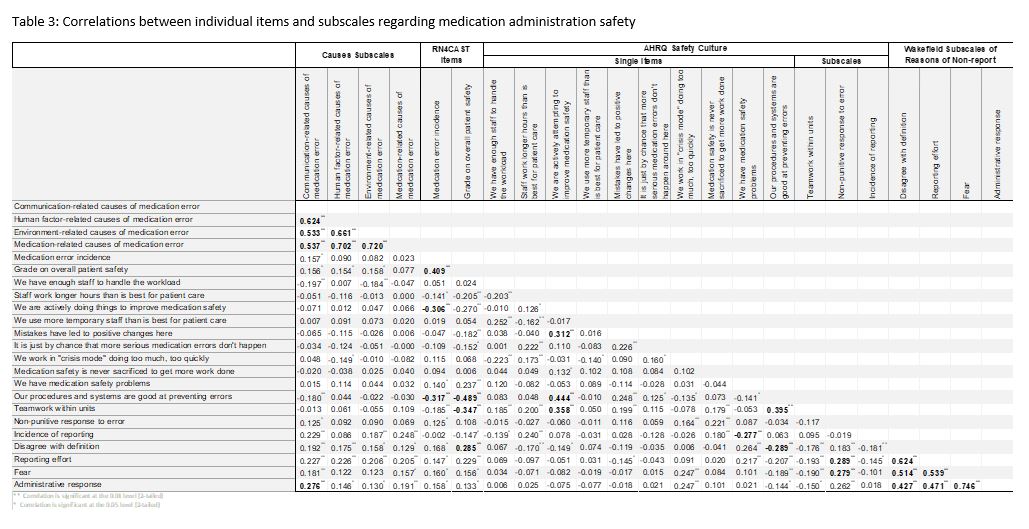
Table 3 presents the correlations between the different individual items and subscales. In these analyses, only findings that are statistically significant (at the 0.05 and 0.01 levels) and have a medium or large correlation are reported on. According to Cohen (1988) the following guidelines can be used for the interpretation of correlations: (a) small r=0.1, (b) medium r=0.3, and (c) large r=0.5.[17]
These results show that ‘Communication-related causes of medication error’ is related to ‘Administrative response’.
Furthermore, the AHRQ safety culture subscales and individual items point to the fact that the items ‘We are actively doing things to improve medication safety’, ‘Our procedures and systems are good at preventing errors’, and ‘Teamwork’ had the most impact on ‘Medication error incidence’ and ‘Grade of overall patient safety’.
Finally, ‘Our procedures and systems are good at preventing errors’ and ‘Non-punitive response’ had the most impact on reasons for non-reporting, and ‘Disagree with definition of medication error’ had the most impact on ‘Medication error incidence’ and ‘Grade of overall patient safety’.
There were no correlations with the demographic data (age, years of experience).
Associations between demographic and hospital data
Regarding demographic data, there was a significant association between female participants and increased reporting of ‘Medication error incidence’ (d=0.60; p=0.05). Also, provincial hospitals had higher scores of the item ‘We use more agency/temporary staff than is best for patient care’ (d=0.66; p<0.001).
Qualitative results
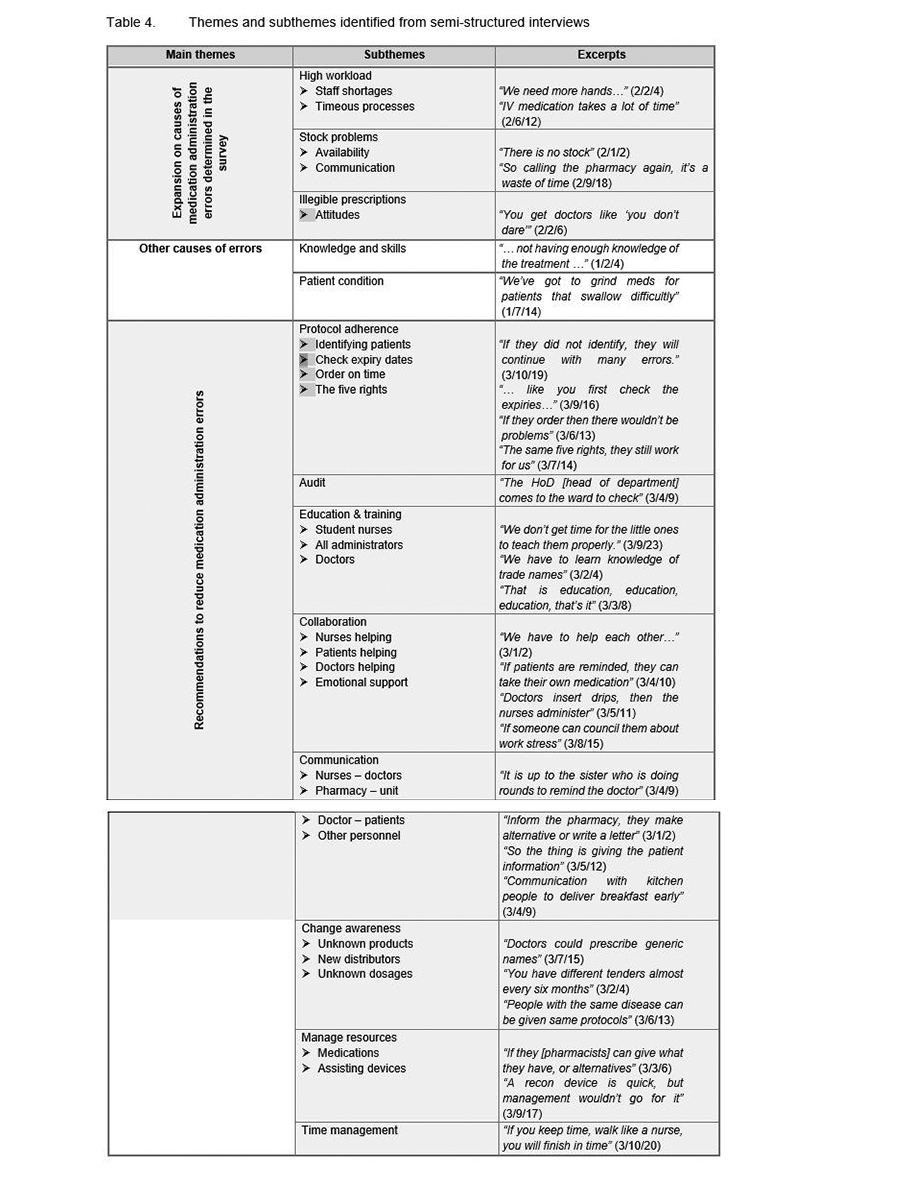
Three themes emerged during thematic content analysis, each with its own sub-themes, which are depicted in Table 4. Three main causes of medication administration errors were identified from the quantitative data, namely high workload, stock distribution problems, and illegible prescriptions. In the qualitative phase these were further explored and identified as theme one, while other causes of medication administration errors were identified as theme two, and recommendations to reduce medication administration errors were identified as theme three.
Several overlaps were recognised between the results from the quantitative phase and the qualitative phase. Figure 1 presents these overlaps, together with recommendations flowing from the integrated findings.
{kind=link}
{kind=link}