Pediatric Immunology and Rheumatology Division at Queen Rania Children Hospital, King Hussein Medical Center, Amman, Jordan, which is the only center in the country has dedicated to pediatric autoimmune disorders, rheumatological disorders, and immune dysregulations, this retrospective study was conducted.
This study aims to describe the clinical characteristics of JIA patients and to characterize our community's clinical characteristics of the disease. To the best of our knowledge, this is the first single-center study that describes the pattern of JIA in Jordanian children.
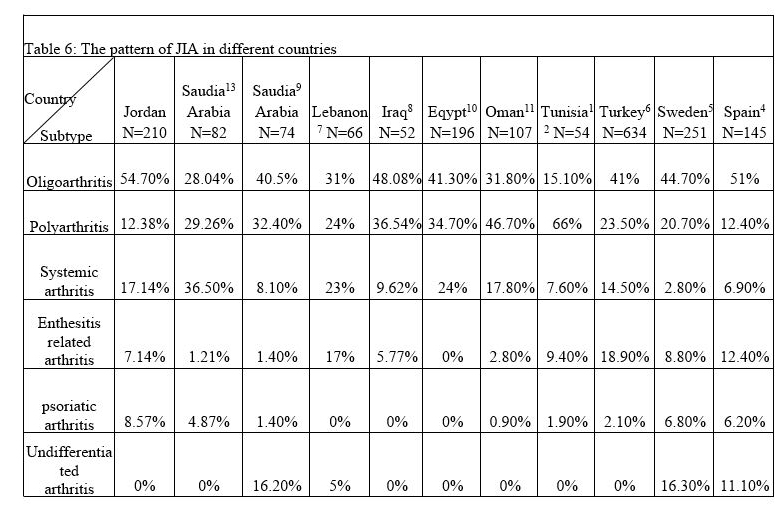
As in previous similar studies, Oligoarticular JIA was the most common subtype, as in Spain (51%), Sweden (44.7%) and Turkey (41%) (4, 5, 6) the Oligoarticular in our cohort was the most common JIA subtype 115/210 (54.7%), Middle East and North Africa (MENA) data showed that Oligoarticular JIA is also the most common subtype as reported in Lebanon (31%), Iraq (48%), Saudi Arabia (40.5%) and Egypt (41.3%) (7, 8, 9, 10).
Unlike similar studies published in Oman and Tunisia where Polyarticular JIA is the most common subtype 46.7%, 66% respectively (11, 12), whereas systemic juvenile arthritis (36.5%) was the most common subtype in another study from Saudi Arabia (13). Table 6 summarizes the published data on JIA patterns in different countries.
The current study reports that the mean age at disease onset was 5.13 ± 3.4 years (range from 7 months to 14 years) which was much lower than that reported by Abou El-Soud et al 10.5 ± 3.6 (range 4–15) years (14), and was close to data published by Bahabri S et al (6 years) (15), and lower than patients of European origin as published by Saurenmann et al 6.5 years (6.1–6.8 years) (16) this observation might be explained by the lower range of the pediatric population of our cohort, as pediatric patients are seen till the age of 14 years at our hospital, then they have referred to adult service. The current study showed female predominance 116/210 with a male to female ratio 1:1.2, a higher ratio was published by E. Solau-Gervais et al, 1:1.7 (17).
Antinuclear antibody (ANA), was positive in 33.6% of cases. Although others such as Khuffash et al (18) and Ozdogan et al (19) mentioned lower results (12%, 5% respectively). This observation reflected on the increased incidence of uveitis. Among oligoarticular JIA cases, the number of ANA-positive patients was 61/115 (53%), which was Close to a study conducted by Al Wahadneh et al 50% (20).
Oligoarthritis is overwhelmingly a disease of the lower limbs, with the knee joint for the most part affected, trailed by the lower limbs with ankle most affected. (21) Similar to the international data the Pattern of joint involvement in Oligoarticular JIA in our cohort showed a predominance of lower limb involvement with knee and ankle involved in 100%, 17.8% respectively, similar joint involvement was found in polyarticular JIA with knee and ankle were involved in 100%, 66.6% respectively. In our dataset, elbow, knee, ankle, and uveitis manifestations were more common in patients with oligo JIA (Fig. 2). When comparing these manifestations between pairs of the 3 subgroups, we concluded that elbow manifestations were not significantly influenced by the subgroups, while wrist, ankle, knee, and uveitis manifestations were dependent on the subgroups compared. Lower odds of presenting wrist, knee, and ankle manifestations were seen in oligo JIA, while uveitis had higher odds in being present in these patients.
Extra-articular manifestations in systemic-onset JIA was fever and reported in 100%, followed by skin rash 66.6%, and the pattern of joint involvement showed upper and lower joints involvement with knee and ankles arthritis reported in 100% and 50%, while elbow and wrist involvement 28% and 55.5% of cases. When comparing these findings with other published data in Egypt (22), we reported a higher incidence of both extra-articular and articular manifestations in systemic-onset JIA.
Uveitis reported in 30/210 (14.2%) and was close to results published by Angeles-Han et al 11.6%. (23). Oligoarticular was the commonest subtype complicated with uveitis 25/115 (21.7%), and positive ANA found in 16/25 (64%). According to one study from Saudi Arabia, uveitis affects 8.1% of oligoarticular JIA (24). Another large population-based study in Germany of JIA patients; uveitis occurred in 12% of all JIA types (25% extended Oligoarticular and 16% persistent Oligoarticular) (25). However, it is not clear if this complication is due to the high prevalence of Oligoarticular JIA or not.
Macrophage activation syndrome (MAS) is a life-threatening complication of systemic juvenile idiopathic arthritis (26), it occurred in our cohort in two patients 2/210 (0.9%), while a higher incidence (33.9%) of this serious complication was reported by Çakan et al (27).The author explained this high rate of MAS in the study by that the institute where the study conducted is a referral center for pediatric rheumatology and a high Percentage of Mediterranean fever (MEFV) gene mutation carriers which may increase the possibility of developing more autoinflammatory disorders than other healthy Population.
JIA treatment aims to reduce the pain, gain joint function, preserve muscle strength, and to avoid systemic complications (28). Although there is no consensus on JIA treatment, but there are many guidelines released from different rheumatology societies or colleges. NSAIDs have traditionally been the mainstay treatment for all kinds of JIA during the First 4 to 6 weeks of the initial treatment either alone or with combination with Intra-articular steroid injection. In case of inadequate response; DMARD was started, and methotrexate (MTX) is the most common DMARD used, and in case of failure, no response or intolerance a switch to another DMARD or add on Biological agent is introduced. (30, 31)
Non-steroidal anti-inflammatory drugs (NSAIDs) were used in 174/210 (82.8%) oligoarticular 103/115 (89.2%), systemic JIA 35/36 (96.7%), at diagnosis or during their disease course. A higher percentage of 99% of oligoarticular JIA patients in central Italy received NSAIDs (29).
Methotrexate is cornerstone treatment in Oligoarticular, polyarticular JIA and in systemic JIA with articular inflammation predominance (32), in our cohort, MTX was used in 81.4% of cases 76.7% of oligoarticular JIA,100% in polyarticular and 90% in systemic arthritis, while MTX was used in 66% of cases in Omani study (11). Other DMARDs were used in cases of MTX toxicity or intolerance, leflunomide 6/210 (2.8%), Sulfasalazine 2 (0.95%), myfortic (MMF) were used in one patient, hydroxychloroquine was used in 4/210 (1.9%) of cases.
Biological treatment found to be safe and effective in severe JIA or refractory cases to synthetic DMARDs (33), in our cohort biological agents were used in 105/210 (50%), and they include Anti-TNF (Tumor necrosis factor) which is a cytokine play role in the pathogenesis of JIA and found in increased levels in the synovial fluid. Tocilizumab a monoclonal antibody directed against IL-6 receptor; increased serum levels found in systemic arthritis, Anakinra is a human recombinant IL-1 receptor antagonist and play a role in the pathogenesis of JIA and is a preferred treatment of systemic arthritis, Rituximab is a human monoclonal antibody directed against CD20 lymphocytes leading to increase B-cell apoptosis and decrease mature B cell expressing CD20 (34), anti-TNF drugs were used in our cohort in 74/210 (35.2%) in which infliximab was the commonest anti-TNF used 30/210 (14.2%), followed by Etanercept 25/210 (12%) while Adalimumab was used in 15/210 (7.1%) and Golimumab in four patients (1.9%). when compare our results in using biological DMARDs with regional data as in Saudi Arabia9, where biological DMARDS were used in 28.4%, with adalimumab being commonest biological treatment, this difference could be explained by that our cohort is larger and the easy accessibility to biological treatment when applying the treat to target strategy. Thirty-eight patients (18%) in our cohort used more than one biological agent, and this group of patients reflects the more severe course in our cohort, and most of them switched to another biological agent due to the inefficiency of the previous agents
Tocilizumab was used in 8% (17/210 of them thirteen patients with systemic arthritis), Anakinra (IL-1 antagonist) was used in one patient (0.5%) with systemic arthritis, Rituximab was used in 8/210 (3.8%) five patients were with systemic arthritis resistant to immunosuppressive, steroid and other conventional biological treatment. A study done by E. Alexeeva et al (35) showed that rituximab may be effective in severe systemic arthritis that is resistant to immunosuppressive treatment and glucocorticoid therapy and other biological treatment.
{kind=link}