Setting
The East Harlem Health Outreach Partnership (EHHOP) is a student-run and faculty-supervised clinic affiliated with the Icahn School of Medicine at Mount Sinai in New York, NY. Established in 2004, EHHOP provides free primary care to East Harlem adults (22 years and older) who are unable to obtain health insurance, most often because they have not met legal residency requirements. In 2018, 12% of East Harlem adults reported not having insurance [18], and a 2017 study estimated that there were at least14,000 immigrants living in East Harlem who did not meet residency requirements [19]. Compared to most other NYC neighborhoods, East Harlem has higher rates of unemployment, violent crime, and premature death and a rate of psychiatric hospitalizations that is three times the NYC average [18]. Demographically, 50% of East Harlem residents identify as Hispanic and 30% as black [18].
Approach to the evaluation and treatment of psychiatric disorders
The EHHOP Mental Health Clinic (E-MHC) is a co-habiting clinic that accept patients who receive primary care at the main medical clinic of EHHOP. Interdisciplinary management is key to its success, as student clinicians in the primary care clinic and E-MHC co-manage patients with a high prevalence of complex medical disease and psychiatric illness.
At initial intake to EHHOP and at least once annually, patients are screened for depressive and anxiety disorders using the Patient Health Questionnaire-9 (PHQ-9) [20] and the Generalized Anxiety Disorder-7 Scale (GAD-7) [21], respectively. Patients with positive screening results on either measure or who otherwise express mental health concerns are referred to the E-MHC for further evaluation and treatment as necessary; those who do not wish to receive care in the E-MHC are sometimes managed by the EHHOP primary care clinic. Clinical services provided to E-MHC patients include psychiatric assessment, medication management, non-specific supportive counseling, and individual psychotherapy conducted by supervised medical student trainees. New patients are seen at least once monthly for medication management and more frequently if they are receiving psychotherapeutic interventions. After stabilization, a minority of patients are transitioned to bi-monthly or quarterly follow-up visits.
Fourth-year psychiatric residents, volunteer psychiatrists, and supervising clinical psychologists oversee the services provided by second to fourth year medical students or MD-PhD students who have completed the first year of medical school. Following all E-MHC patient appointments, the student trainees present their patient to a supervising psychiatrist or fourth-year resident in psychiatry. Initial diagnoses are based upon unstructured interviews by the student, who then finalizes the diagnostic formulation with the supervising psychiatrist or resident. Supervisors review the patient’s status, formulate a treatment plan with the student, and provide additional mentoring in outpatient psychiatry. After these discussions, both the student and the supervisor meet with the patient to answer questions, review the assessment and treatment plan, and ensure that there are no safety concerns.
Patients expressing suicidality at any time are given a more thorough risk assessment by the supervisor; if needed, patients are taken to a nearby emergency room for continued monitoring and stabilization. As needed, on-call psychiatry and medical faculty supervise trainees who triage phone calls; faculty provide necessary navigation of care and communication with emergency room and inpatient teams.
Psychotropic medications are prescribed under the supervising psychiatrist, and patients receive their medications with no out-of-pocked costs either at a Mount Sinai pharmacy or on-site immediately after their appointments [16]. Of note, there is a limited formulary of medications stratified by cost on a web-based application that providers consult when prescribing medications. In between the Saturdays on which the E-MHC is open, first and second year medical and graduate students manage the clinic’s schedule and coordinate follow-up visit and appointment reminders for all patients.
Collection of socio-demographic and clinical variables
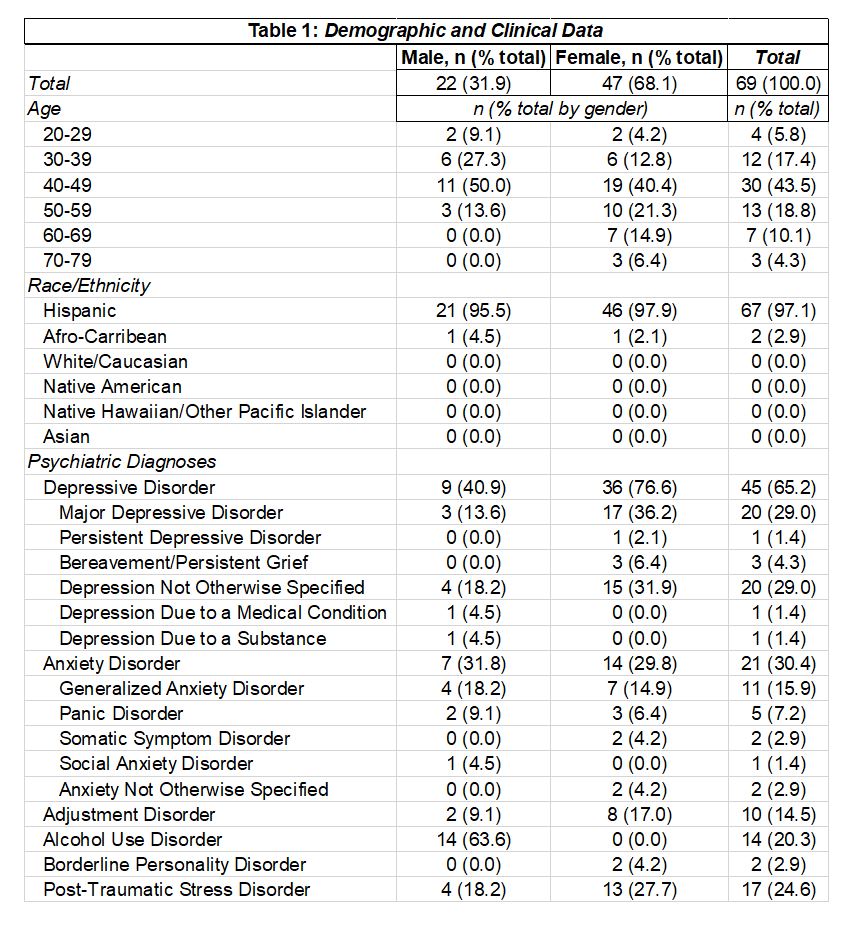
Age, race/ethnicity, and gender (male or female) were identified by review of patients’ electronic medical records from January 1st, 2009 to March 1st, 2020. Psychiatric diagnoses were collected from the patient’s charts and confirmed in provider notes; patients could have multiple diagnoses if they were concomitantly diagnosed or if different diagnoses were listed throughout the course of treatment. Psychiatric diagnoses collected included major depressive disorder, persistent depressive disorder, seasonal affective disorder, depression not otherwise specified (NOS), generalized anxiety disorder, panic disorder, social anxiety disorder, somatic symptom disorder, anxiety not otherwise specific (NOS), adjustment disorder, post-traumatic stress disorder (PTSD), borderline personality disorder, substance use disorders, and persistent complex bereavement disorder. For all statistical tests, major depressive disorder, depression NOS, persistent depressive disorder, seasonal affective disorder, and persistent complex bereavement disorder were combined into a single diagnostic group termed “depressive disorders.” Similarly, generalized anxiety disorder, panic disorder, social anxiety disorder, and somatic symptom disorder were combined into a composite diagnostic category of “anxiety disorders.” We also collected information about current and past sexual assault and intimate partner violence (SA/IPV) based upon review of provider notes.
Evaluation of clinical performance on behavioral healthcare service measures
We evaluated the quality of clinical care at the E-MHC using the Healthcare Effectiveness Data and Information Set (HEDIS) performance metrics established by the National Committee on Quality Assurance. Many previous studies of clinical care performance utilize the HEDIS metrics, as they are empirically derived and objectively defined measures with specific criteria designed to operationalize each aspect of healthcare performance [22]. We selected HEDIS behavioral healthcare metrics based upon those that were relevant to the clinical services provided by the E-MHC in the year 2019 and that could be calculated using the metric’s definition and the availability of patient data. Based upon the available data, we were able to compare our performance on metrics related to optimal provider contacts for treatment of depressive disorders, receipt of effective acute- and continuation-phase antidepressant treatment, smoking cessation interventions, and follow-up care after ED visits for alcohol and other drug dependencies (AOD). We compared the proportions of E-MHC patients who did and did not meet the metric satisfaction criteria to the same proportions reported for various New York State (NYS) managed care groups collected from published reports by the NYS Department of Health [23–25]. For the effective antidepressant medication management acute- and continuation-phase metrics, we also included our previously published data [15] in the comparisons to determine if the E-MHC’s performance improved over time. Due to the small sample size in our study and the unbalanced groups, Fisher exact tests were used to quantify the likelihood of a patient having met the specific metric criteria between the E-MHC 2019 data and each of the additional comparator groups. Results are reported as odds ratios with 95% confidence intervals (CIs) and were considered significant if p < 0.05.
Assessing the extent to which depressive and anxious symptoms improve over time
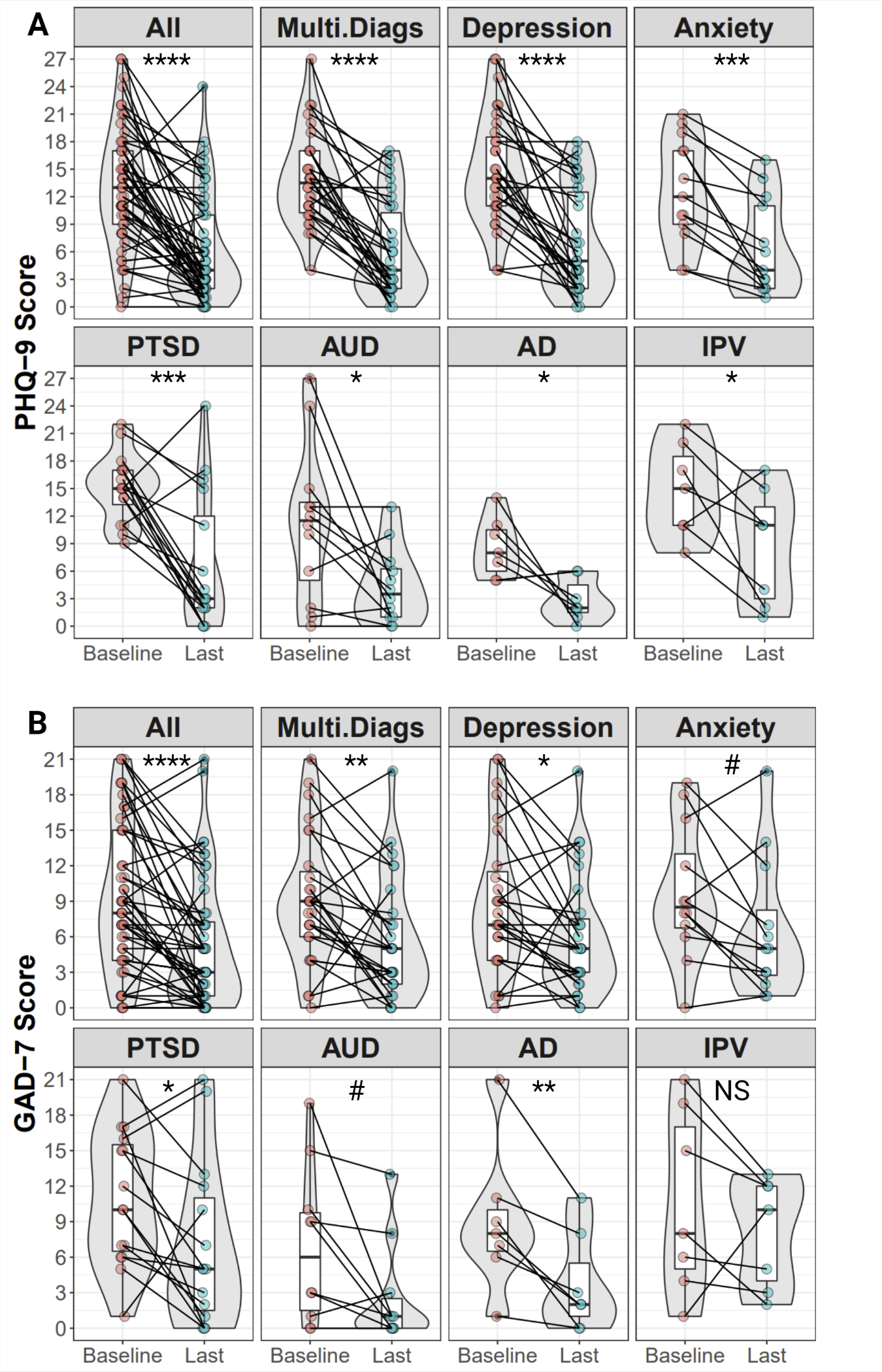
We longitudinally assessed depressive and anxious symptoms using the PHQ-9 and GAD-7, respectively, which were available from patients’ charts as part of routine care and symptom monitoring in the clinic. We first defined baseline symptom scores as either the score upon referral to the E-MHC or the score(s) reported at the initial assessment visit. Patients who had neither and had no scores reported within the first month of treatment were excluded from the analyses. End-point scores were defined as those achieved at the last recorded visit for the patient within the study period. For each symptom-based measure, we generated two models, each with differing aims:
(1) We first sought to evaluate the extent to which patients’ depressive and anxious symptoms improved over the course of their treatment in the E-MHC. Linear mixed effects (LME) models were derived to ascertain whether the number of treatment sessions in the E-MHC was associated with symptom improvement, along with factors that may affect improvements over time. In the exploratory analyses, initial models were built with PHQ-9 or GAD-7 score as the dependent variable with session number as the fixed effect and patient ID as the random effect, accounting for the many non-controlled factors specific to each patient. Subsequently, additional fixed effects were added (see below) and the resulting models were selected using a Bayesian Information Criterion (BIC) score, a measure of how much each model explained while also penalizing for overfitting [26].
(2) We generated logistic regression models to identify what factors, if any, were associated with the probability of a patient achieving a clinically significant improvement in symptoms at the endpoint time. “Clinically significant improvement” (CSI) was defined as a reduction in the magnitude of symptoms (separately on each measure) of at least 50% [26, 27]. Candidate logistic regression models were selected using all subsets regression with the bestglm() function of the bestglm package [28]. The model with the best BIC score was selected. Finally, we graphically illustrated model predictions using the predict() function in R.
For all models, we only included those who had at least mild PHQ-9/GAD-7 symptoms at baseline, defined as a score of 5 or greater for both scales [20, 21]. Potential predictor variables tested included age, gender, baseline PHQ-9 score, baseline GAD-7 score, whether the patient had more than one psychiatric diagnosis, the number of psychiatric diagnoses at baseline, the number of visits in the E-MHC, and whether the patient was listed as having (Y/N) depression, anxiety, adjustment disorder, alcohol use disorder, post-traumatic stress disorder, and/or intimate partner violence.
Evaluation of Patients Feedback
We created a custom Patient Feedback Survey based upon frequently asked questions in the research literature on scales measuring patient satisfaction with mental health services [29]. All questions were asked on a 5-point scale with possible answers of “Strongly Disagree,” “Disagree,” “Neutral,” “Agree,” and “Strongly Agree.” All feedback surveys were collected at the end of patient visits, and some patients completed the survey more than once over the course of their overall treatment in the E-MHC. Copies of the survey in both English and Spanish are provided in Supplementary File 1.
{kind=link}
{kind=link}