Overall, we found it useful to synthesise health service implementation barriers using both data-driven and theory-driven methods to gain a comprehensive understanding of the barriers to childhood vaccination. The data-driven categories represented the review data in a clearer way than the theoretical domains, with better differentiation; but the four missing theoretical domains were useful as a way to identify key gaps to be addressed in the item pool for developing a new tool to diagnose the causes of childhood under-vaccination.
Resolving conflicts at the domain level was relatively easy, with 100% agreement reached quickly for the most relevant domain. However there were some barriers that could have been placed in 2 or 3 domains, e.g. previous experience of vaccine side effects could be framed as knowledge, beliefs or salient events. Resolving conflicts at the construct level was more difficult because many constructs within a domain were very similar when applied to the brief barrier descriptions extracted from reviews, for example the influence of family member opinions could fit within group identity, social norm or social pressure. The decisions made at construct level were arguably more subjective than the domain level, but both needed to be considered to make sense of many barriers that could be framed in different ways.
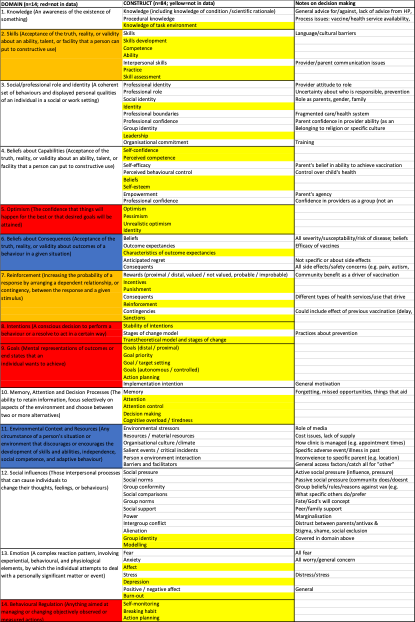
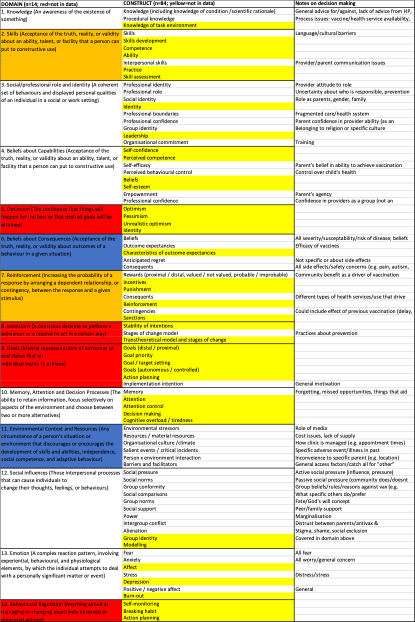
For this study it was necessary to go into more theoretical detail than the commonly used models: the COM-B and TDF. Importantly, the gaps identified in our data-driven review would not have been found if the analysis had only been done at the COM-B level, as all six components were addressed by the 10 data-driven domains. In addition, the 14 TDF domains were still not specific enough for two coders to reliably map the barrier data so we were required to go back a step to the 84 theoretical constructs that informed the TDF development. We found it helpful to use a combination of domain and construct level to map the data. A previous review using the TDF identified some issues that could not be mapped to the TDF (e.g. clinician and patient characteristics), but some of these could be mapped at the construct level depending on the framing, e.g. under professional identity, skills, environment x person and resources constructs12.
This paper provides a methodology for anyone seeking to understand an implementation issue that already has a large amount of qualitative and/or quantitative research – complementing an earlier paper that focuses on how to apply the TDF in primary qualitative research 6. There are several practical implications for other researchers seeking to comprehensively understand implementation barriers using theoretical models in this way. Firstly, you need to decide on very specific framing for a health situation, e.g. only looking at the parent perspective on vaccinating their child determines how you frame barriers relating to the doctors’ knowledge. Conducting this process from the health professional perspective would produce different results in terms of the theoretical constructs identified in the literature. Secondly, the COM-B model was not specific enough with uneven explanation of different barrier types; so you may need to go into more detail at domain and construct level to interpret the data. Thirdly, theory was useful for identifying gaps in a data-driven review of literature, but data driven categories made more sense for the specific implementation topic. So the value of using a theory-driven approach may depend on the purpose of conducting the review. For our purposes, this review will inform the development of a diagnostic tool to measure the causes of under-vaccination, requiring us to include the widest possible range of behavioural drivers. For other projects, it may be more prudent to focus only on the theoretical drivers that are within an organisation’s control to address, or to identify data-driven issues from the perspective of key stakeholders to ensure their interest and support.
More generally, this study has implications for theoretical models commonly used in implementation science. Some constructs are vague and became catch alls – e.g. barriers and facilitators in this case. On the other hand some constructs are too specific and hard to distinguish – e.g. group vs social norms, so it makes sense to combine this into one TDF domain. In our experience, the decision was often between constructs in different domains, rather than constructs within a domain, suggesting that there are some issues with the way the TDF domains are differentiated. On the other hand, the construct level was often too subjective and detailed to identify clear gaps in data. This suggests that overarching models like the COM-B and TDF need to be supplemented with more context-specific models for different health areas (e.g. prevention versus treatment of infectious disease), targets of behaviour change (e.g. parents versus doctors), and the context (e.g. higher resource settings where psychological barriers may be more important, versus lower resource settings where practical access issues require greater differentiation). Another option would be to use broad implementation frameworks that include practical issues like cost, such as the Consolidated Framework for Implementation Research (CFIR)13. Other researchers have found it helpful to combine the TDF and CFIR for a more comprehensive approach14. A third option would be to add more specific domains to the next version of the TDF to better differentiate between issues relating to “Environmental Context and Resources”. In our review, this covered a very wide range of issues: socio-economic issues such as having low income, societal issues like the influence of media, health system issues like vaccine supply and cost, and individual access issues like distance and time. This was found to be a catch all category in many previous reviews of clinicians and patients using the TDF12,15–19, so is not limited to the issue of vaccination barriers. For example, a review of barriers to low back pain guidelines found this domain was common to 4/5 clinician behaviours while many other domains were not covered at all17. Another review on diabetic screening identified 17 barriers in this domain versus 6 for the next most common domain15. Further development of this construct may need to be specific to different health topics.
The TDF domains that weren’t covered well by the vaccination barrier review data – optimism, behavioural regulation, intentions and goals – may have been found in other areas of the literature. Optimism is often researched as a personality-based predictor of health20, and this conceptualisation is unlikely to be identified as a public health barrier or the target of a public health intervention. Behavioural regulation may not relate as well to occasional behaviours like vaccination, compared to something like eating healthy food, which requires daily monitoring21. Intentions and goals may be more likely found in theory-based intervention literature where intention is a common outcome22, rather than the barrier literature where intention is conceptualised more as a product of the barriers. These domains may be appropriate to understand other health contexts, but for this case study they were less relevant. However, the low prevalence of these domains appears to be similar to some previous barrier reviews on different topics (e.g. the reviews on low back pain guidelines and diabetic screening described above15,17).
This study addressed reliability by using a method of independent coding using both inductive and deductive approaches. Our team included a wide variety of expertise to help contextual framing for theoretical constructs as applied to data-driven barriers. The limitations include restricting our review data to parent barriers only, which affected the way that health professionals’ and heatlh system barriers were conceptualised. We also applied only one overarching framework to behaviour change models, and acknowledge that there are many other approaches to this theoretical issue.
In conclusion, using both data and theory approaches can help achieve a more comprehensive understanding of health service implementation problems. However, the process is subjective so requires a wide range of expertise to reduce biased interpretation and to maximise utility of the identified barriers for the specified purpose.
{kind=link}
{kind=link}