Ethics approval
The ethics committee of Beijing Hospital approved this retrospective study (2017BJYYEC-080-02) and waived the need for obtaining patients’ informed consent, given the retrospective nature of the study.
Participants
This was a retrospective, multicenter study conducted in 18 medical centers across China. Participants from 34 hospitals in northern China were included in this study. In total, 1,862 participants hospitalized because of acute exacerbation of COPD between February 2015 and February 2018 were included in this study. We excluded participants without complete data on baseline characteristics, comorbidities, or administered medications during the last year. We reviewed the electronic patient medical records for information regarding symptoms, tests, hospitalization treatment, and prognosis. Subsequently, we reviewed computed tomography (CT) results and pathogen identification tests (including sputum smears, sputum cultures, and fungal cultures). An additional figure details the selection of the included patients (see Additional Fig. 1).
Right heart failure was diagnosed by cardiologists according to the following criteria of the European Society of Cardiology: isotopic ventriculography when the right ventricle ejection fraction was ≤ 35 and /or in exercise decreased at least 5% with respect to rest value and typical signs (hepatojugular reflux, edema, and ascites). [12]
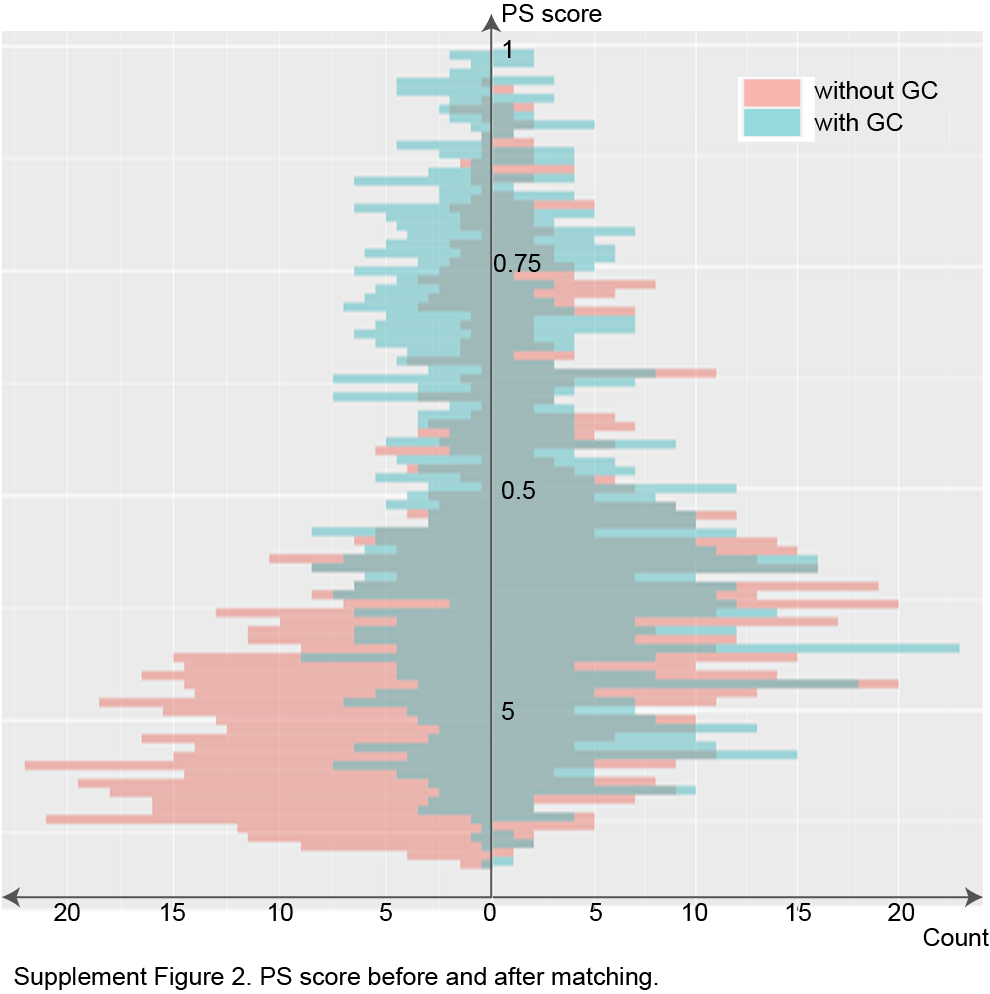
Baseline characteristics and propensity score-matching
Based on the regularity of inhaled glucocorticoid usage over the past year, patients were divided into the glucocorticoid (with-GC, n = 763) and without-glucocorticoid groups (without-GC, n = 1099). First, we compared the baseline characteristics, comorbidities, and medications taken during the past year between the two groups. Second, the baseline characteristics, comorbidities, and medications patients used in the past year were matched using 1:1 PSM; therefore, we obtained a matched cohort of 556 patients per group. Third, to detect the effect of PSM, we compared the above factors between the two matched groups.
The baseline characteristics included age, body mass index (BMI), sex, smoking history, acute exacerbation frequency, forced expiratory volume in 1 s to forced vital capacity ratio, and late-stage COPD. Matched comorbidities included asthma, pulmonary thromboembolism, interstitial lung disease, bronchiectasis, tuberculosis, coronary artery disease, coronary heart disease, diabetes, high blood pressure, cardiovascular disease, and anxiety. Medications that patients used in the last year were also matched and included short-acting beta antagonists, short-acting muscarinic antagonists, LABA, long-acting muscarinic antagonists (LAMA), theophylline, antibiotics, expectorants, and traditional Chinese medicines. Propensity scoring and 1:1 matching were conducted using the MatchIt package (version 3.0.2) for R software version 3.6.2 (https://www.r-project.org/)
Symptoms and in-hospital tests
Respiratory symptoms, cyanosis, accessory respiratory muscle involvement, unstable hemodynamics, right heart failure, and consciousness disturbance were collected by reviewing the admission records of patients. This analysis included the results of the first laboratory tests after admission. Respiratory failure (RF) was defined as an arterial partial pressure of oxygen to the fraction of inspired oxygen ratio < 300 mmHg. Type I RF was defined as an RF with a partial pressure of carbon dioxide (PaCO2) < 50 mmHg, and Type II RF was defined as an RF with PaCO2 > 50 mmHg. Symptoms and tests were compared before and after PSM.
The results of the CT imaging and pathogen tests were first obtained after admission, before any treatment. The positions of the lung lesions were recorded. Qualified pathogen tests, including sputum smear, culture, and fungal culture, were also reviewed. Qualified pathogen tests indicated a white blood cell count > 25 and squamous cells < 10 in the sputum. After comparing the differences between CT and pathogen tests between the two groups in the original cohort, we performed PSM separately to match baseline characteristics. Subsequently, we compared the CT imaging findings and pathogen tests between the two matched groups.
Treatments and prognosis
Treatments in the general wards, including both drug and non-drug treatments, were reviewed. Drug information included antibiotic types used at the time, the duration of antibiotics used, and whether systematic glucocorticoids were used. Non-drug treatments, including oxygen therapy and non-invasive positive-pressure ventilation, were also reviewed.
Statistical analyses
Statistical analyses were performed using the R software version 3.6.2. Categorical variables are reported either as numbers (n) or proportions (%), and continuous variables are expressed as either means (standard deviations) or medians (interquartile ranges). Student’s t-test was used for comparisons of continuous variables; otherwise, the Mann–Whitney U test was applied. Categorical variables were compared using the chi-squared (χ2) test with Yates’s correction or Fisher’s exact test (when the total sample was < 40 or the expected frequency was < 1). A comparison between patients who did and did not use glucocorticoids was conducted.
{kind=link}