Design
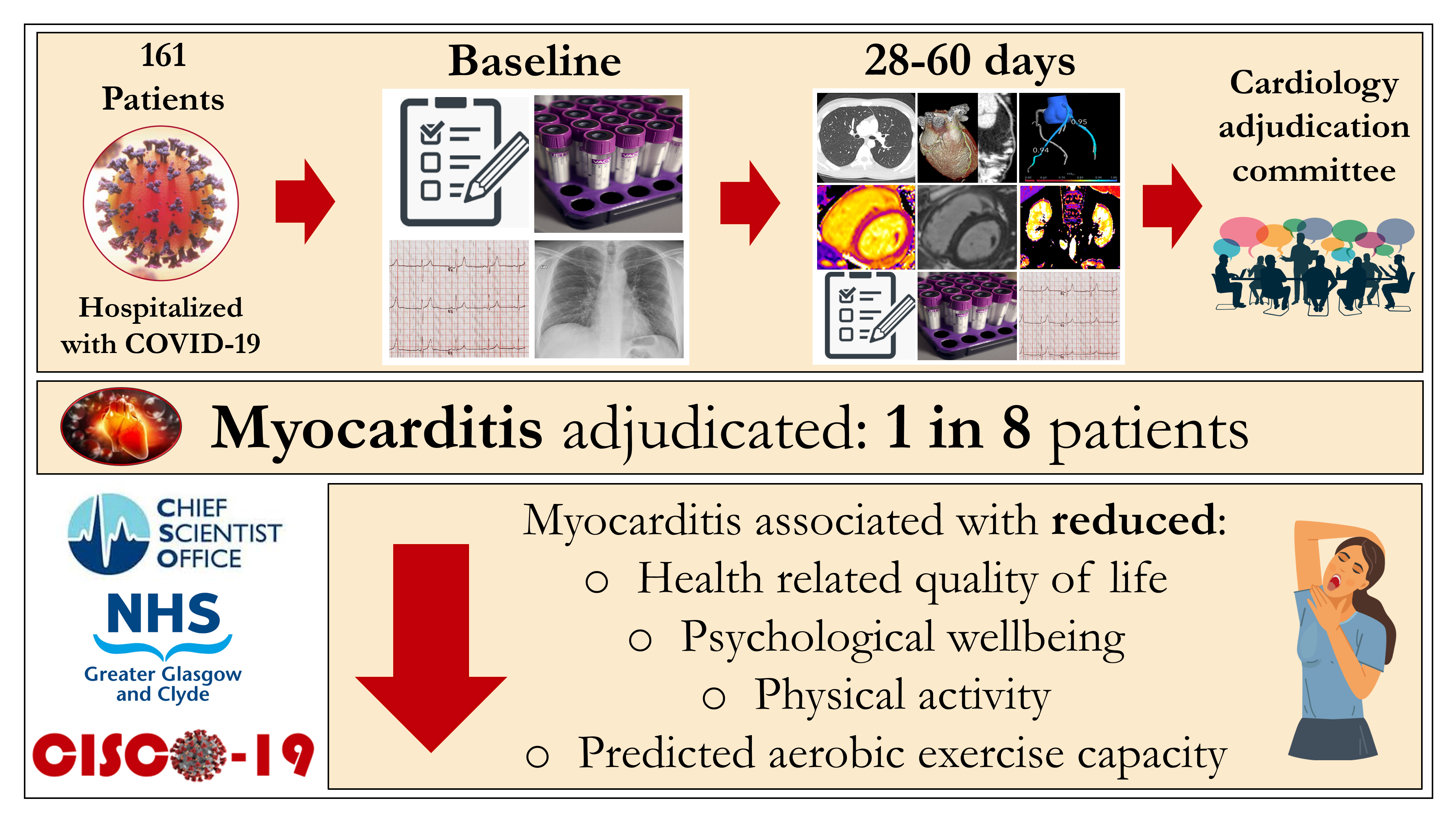
This study involved a prospective, observational, multicenter, longitudinal, secondary care cohort design to assess the time-course of multiorgan injury in survivors of COVID-19 during convalescence. Clinical information, a 12-lead digital ECG, blood and urine biomarkers, and patient reported outcome measures were acquired at enrolment (visit 1) and again during convalescence, 28–60 days post-discharge (visit 2). Chest computed tomography (CT), including pulmonary and coronary angiography, and cardio-renal MRI were acquired at the second visit.
Setting
The study involved three hospitals in the West of Scotland (population 2.2 million) - the Queen Elizabeth University Hospital, the Royal Infirmary in Glasgow, and the Royal Alexandra Hospital in Paisley.
Participant identification
Patients who received hospital care for COVID-19, with or without admission, and were alive, were prospectively screened in real time using an electronic healthcare information system (TrakCare®, InterSystems®, USA) and daily hospital reports identifying inpatients with laboratory-positive results for COVID-19.
Eligibility criteria
The inclusion criteria were: (1) age ≥18 years old; (2) history of an unplanned hospital visit e.g., emergency department, or hospitalization >24 hours for COVID-19 confirmed by a clinical diagnosis, laboratory test (e.g., polymerase chain reaction (PCR)), and/or a radiological test (e.g. CT chest or chest radiograph); (3) ability to comply with study procedures; and (4) ability to provide written informed consent. The imaging results were reported by accredited radiologists according to contemporary, national guidelines20.
The exclusion criteria were: (1) contra-indication to magnetic resonance (MR) imaging (e.g., severe claustrophobia, metallic foreign body); and (2) lack of informed consent.
Screening
A screening log was prospectively completed. The reasons for being ineligible, including lack of inclusion criteria and/or presence of exclusion criteria, were recorded.
Diagnosis of COVID-19
A diagnosis of COVID-19 was based on either laboratory evidence of SARS-CoV-2 infection using a PCR test (Roche Cobas 6800 or Seegene SARS-CoV-2 PCR) on a biospecimen or a radiological and clinical diagnosis of COVID-19 but biospecimen negative 21.
Diagnosis of myocardial injury
The diagnosis of myocardial injury aligned with the Fourth Universal Definition of Myocardial Infarction22. Troponin I was measured in hospitalized patients using the Abbott Architect STAT TnI assay (sex-specific >99th percentile upper reference limit: female: >16 ng/L, male: >34 ng/L.
Diagnosis of acute kidney injury
Acute kidney injury (AKI) was defined as any stage of AKI (1-3) during COVID-19 hospitalization using categorization with the Kidney Disease: Improving Global Outcomes (KDIGO) criteria (Supplement) 23.
Research schedule
The protocol involved two visits. The first visit involved informed consent and baseline assessments during the initial hospitalization, or as soon as possible after discharge. The second visit occurred 28–60 days post-discharge. This window was positioned to reflect the convalescent phase and give sufficient scope to schedule the patients.
The procedures involved prospective collection of clinical data and a time-course of research investigations. Clinical data included demographics, medical and cardiovascular history, findings from clinical examinations, laboratory and radiological tests, cardiology tests (including an electrocardiogram (ECG) and an echocardiogram if available) and treatment. The research investigations at both visits included blood and urine samples, a 12-lead digital ECG (Beneheart R3, Mindray, Huntingdon, UK), health status questionnaires, and assessments of adverse events (Supplement). Heart, lung, and kidney imaging were acquired at the second visit.
Electrocardiology
SARS-CoV-2 infection and treatment may cause alterations in heart rate and rhythm, and ventricular repolarization. The changes may be specific for myocarditis e.g., concave ST-elevation, or non-specific e.g., ventricular arrhythmias. Digital ECGs were acquired, de-identified and provided to the University of Glasgow Electrocardiology Core Laboratory for automated analysis and adjudication. The ECG features of myopericarditis were predefined according to contemporary criteria17.
Biomarkers
Blood and urine samples were collected at enrolment (visit 1) and 28–60 days post discharge (visit 2). Circulating biomarkers of cardiac injury (troponin I, N-terminal (NT)-pro hormone brain natriuretic peptide (NT-proBNP), inflammation (C-reactive protein, ferritin), thrombosis (TCT ratio, D-Dimer, fibrinogen, Factor VIII, antithrombin, protein C, protein S), endothelial activation (von Willebrand factor (vWF):GP1bR, VWF:Ag) and renal function (serum creatinine, glomerular filtration rate (GFR) was estimated using the Chronic Kidney Disease Epidemiology (CKD-EPI) equation24) and urinary albumin: creatinine ratio), and their changes over time, were investigated. The measurements were undertaken in a central laboratory, blinded to the other clinical data. The methodology is described in the Supplement.
Multimodality imaging
CT
A 320-detector CT scanner (Aquilion ONE, Canon Medical Systems Corp.) provided full heart coverage within a single heartbeat. Intravenous metoprolol was used where required to control the heart rate (target 60 beats/min) and sublingual glyceryl trinitrate was given to all patients immediately before the scan acquisition. An initial low radiation dose helical scan of the thorax was acquired for comprehensive assessment of the lungs. A contrast bolus timing scan was acquired to provide information on cardiopulmonary transit times. Non-contrast and contrast-enhanced angiographic breath-hold ECG-gated volumes were acquired and timed for optimum pulmonary and systemic arterial (coronary) opacification. Patients with severe renal dysfunction underwent non-contrast CT.
Coronary CT angiography provided information on the presence and extent of coronary calcification (calcium score), coronary artery disease, and whether any coronary artery disease was obstructive (flow-limiting) including the Coronary Artery Disease - Reporting and Data System (CAD-RADS) score25. The functional significance of coronary artery disease was evaluated using fractional flow reserve CT (FFRCT; HeartFlow, Redwood City, CA). A FFRCT ≤0.80 defined obstructive coronary artery disease, taking the lowest value in the vessel. FFRCT measurements were taken at prespecified points using standard coronary segment definitions as a reference26. Median FFRCT values were calculated for the left anterior descending, circumflex, and right coronary arteries, respectively, in combination with subsidiary vessels (i.e., diagonal arteries, obtuse marginal arteries). Patient-level FFRCT values included all these coronary arteries.
Pulmonary vascular imaging assessed arterial thrombus (embolism)27. CT was used to delineate pulmonary features associated with COVID infection e.g., atelectasis, reticulation and/or architectural distortion, ground-glass opacity, and pre-existing lung damage e.g., emphysema. Cardiac and extra-cardiac incidental findings were reported and managed according to local standards of care.
Cardiovascular MRI
Cardiovascular MRI was undertaken to measure heart structure and function and assess for persisting evidence of myocardial injury and/or myocardial infarction using multi-parametric techniques28. MRI was acquired in a single reference site for all patients using a research-dedicated 3.0 Tesla (3T) scanner (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) with two 18-channel surface coils placed anteriorly and a 32-channel spine coil placed posteriorly. All patients underwent protocol-directed MRI in the convalescent phase, 28–60 days after discharge. The scan protocol included cine-imaging of cardiac anatomy and function and myocardial tissue characterization using multiparametric techniques. They included 1) mapping myocardial native longitudinal relaxation time (T1 in milliseconds) using the modified Look-Locker inversion recovery technique (T1-mapping) before and after intravenous administration of gadolinium contrast media (0.15 mmol/kg of Magnevist, Bayer Healthcare), 2) mapping transverse relaxation time (T2 in milliseconds), 3) first pass contrast-enhanced perfusion and 4) late gadolinium-enhancement imaging. Specific details on the MRI protocol are provided in the Supplement.
The expert consensus recommendations for the MRI diagnostic criteria of non-ischemic myocardial inflammation (modified Lake Louise criteria) were used to diagnose definite myocardial inflammation (abnormal T2 and T1 (native T1, late gadolinium enhancement or extracellular volume)) or probable myocardial inflammation (abnormal: T2 or T1)17,29 (Supplement). Reference ranges derived from the UK Biobank were used to interpret cardiac structure and function30, and contemporary local reference ranges specifically derived using the 3T MRI scanner (MAGNETOM Prisma) were used to define thresholds for localized abnormalities in myocardial T1- and T2- relaxation times. To limit selection bias, patients with severe renal dysfunction (GFR <45 ml/kg/m2) were not excluded. They were eligible for MRI with or without contrast media according to the site Radiology protocol.
Renal MRI
Multi-parametric renal MRI included anatomical imaging and tissue characterization by measurement of native T1 and T2. The volume (ml), and native T1 (ms) and T2 (ms) in regions of interest obtained within the cortex and medulla of each kidney were recorded, and the averaged value of these parameters for both kidneys was then determined. Corticomedullary differentiation reflects a difference in tissue contrast on T1-weighted imaging due to a shorter T1 relaxation time of the cortex relative to the medulla, this being attributed to differences in water content between the two tissues31,32. Corticomedullary differentiation, reported here as a ratio of T1 cortex divided by T1 medulla32, may diminish in kidney disease31.
Blinding
The patients and the outcome assessors were blinded. Outcome assessments, including laboratory, MRI and CT analyses, and endpoint adjudication were undertaken by blinded researchers. The patients completed the health status questionnaires before undergoing the scans and they were unaware of the test results.
Outcomes
Primary outcome
The predefined primary outcome was a diagnosis of myocarditis (myocardial inflammation), an endotype of acute myocardial injury.
The diagnostic criteria for myocarditis included relevant clinical findings and test results (Supplement)17. Positive clinical findings included chest pain, pericarditic or pseudo-ischemic in nature, new onset breathlessness, subacute/chronic breathlessness, palpitations, unexplained arrhythmia, syncope, aborted sudden cardiac death, or unexplained cardiogenic shock. Positive test findings included 1) ECG features, 2) elevated troponin I (sex-specific >99th percentile upper reference limit: female: >16 ng/L, male: >34 ng/L; Abbott Architect STAT TnI assay); 3) functional and structural abnormalities on cardiac imaging (echocardiography, angiography, or MRI), and 4) tissue characterization MRI, including myocardial edema and late gadolinium enhancement with a distribution in alignment with the modified Lake Louise diagnostic criteria for myocarditis29. Acute and chronic myocardial pathology can be identified, discriminated, and quantified using MRI.
Myocarditis was clinically suspected if at least 1 clinical finding and at least 1 diagnostic test criterion from different categories, in the absence of: (1) angiographically detectable coronary artery disease (coronary stenosis ≥ 50%); (2) known pre-existing cardiovascular disease or extra-cardiac causes that could explain the syndrome (e.g., valve disease, congenital heart disease, hyperthyroidism, etc.). Suspicion increases with a rising number of fulfilled criteria. If the patient was asymptomatic, at least 2 diagnostic criteria were required.
Adjudication of the primary outcome
A diagnosis of myocarditis is susceptible to confounding through ascertainment bias. Recent studies in COVID-19 have not implemented the modified Lake Louise diagnostic criteria18,19. Accordingly, we pre-specified an adjudication procedure for the primary outcome, involving a panel of cardiologists with specialty accreditation. The reviews were undertaken according to a prespecified charter.
Consultant cardiologists (n=14) who were independent of the research team were invited as assessors. They were initially provided with information on the European Society of Cardiology Working Group on Myocardial and Pericardial Disease position statement on myocarditis17, a charter, and training cases. The cardiologists were blind to the identity of the patients and independent of their clinical care. The adjudications were coordinated by a researcher (A.M.) using Teams (Microsoft, Seattle, USA) software.
Each cardiologist independently assessed the clinical data, including the medical history, biomarkers, ECG, and radiology reports for the CT chest, CT pulmonary angiogram, coronary CT angiogram, and cardiac MRI. Deidentified source clinical data e.g., scan images, were made available on request. The cardiologists determined the likelihood (not likely / unlikely / probable / very likely) of myocardial inflammation (myocarditis). The final diagnosis was based on the median likelihood based on the adjudications of 5 cardiologists. Their determinations were also categorized in binary form (not/unlikely = no; probable/very = yes).
Secondary outcomes
The differential etiology of myocardial injury/inflammation was adjudicated as a secondary outcome. The potential endotypes were:
1) SARS-CoV-2 myocarditis,
2) Acute stress cardiomyopathy,
3) Myocardial ischemia/impaired perfusion as a stressor of inflammation,
4) Infective myopericarditis (non-COVID infection),
5) Drug-induced (toxic) myocardial inflammation,
6) Idiopathic myocardial ± pericardial inflammation.
The endotypes of acute myocardial injury, including the type of myocardial infarction according to the 4th Universal Definition of MI22, and myocarditis (myocardial inflammation, ischemia or stress cardiomyopathy)17,29, were secondary outcomes.
Renal outcomes
Renal function was assessed using convalescent eGFR (CKD-EPI24) and albuminuria. Multi-parametric renal MRI at 28-60 days provided information on renal parenchymal disease.
Health status and patient reported outcome measures
Questionnaires were completed by participants at enrolment (visit 1) and 28–60 days after the last episode of hospital care (visit 2), blind to the other research data. Self-reported health status was assessed using the generic EuroQOL EQ-5D-5L questionnaire and the Brief Illness Perception Questionnaire (Brief-IPQ)33,34. The Patient Health Questionnaire-4 (PHQ–4) was utilized to assess for anxiety and depressive disorders35. The Duke Activity Status Index (DASI) was used to assess predicted maximal oxygen utilization (ml/kg/min), a measure of aerobic capacity, and functional capacity, a higher score reflects greater physical function36. The International Physical Activity Questionnaire - Short Form (IPAQ-SF) measures the types and intensity of physical activity and sitting time that people do as part of their daily lives. The score reflects total physical activity in metabolic equivalent minutes per week37.
Longitudinal follow-up
The participants were invited to give consent for clinical outcome assessment during follow-up using electronic health record linkage without direct contact.
Statistics
The statistical analyses were pre-defined in a Statistical Analysis Plan.
Sample size calculation
The primary outcome was myocarditis (myocardial inflammation), and the primary analysis determined the proportion of patients with the primary outcome by visit 2. The likelihood of myocarditis was determined based on the median likelihood from the clinical adjudication committee. To detect an association between a history of pre-existing cardiovascular disease and incident myocardial inflammation (myocarditis), we assumed a 25% prevalence of prior cardiovascular disease in the study population, and the incidence of myocardial inflammation in those with/without prior cardiovascular disease to be 33% and 10%, respectively38. To have 80% power to detect this difference we calculated that 140 participants (35 with cardiac problems, 105 without) with complete data would be required. Anticipating that 10-15% of the participants may have incomplete imaging e.g., artefact or claustrophobia, the target sample size was 160 to complete the imaging visit.
Cardiovascular disease status was prespecified and defined by (1) a prior history of cardiovascular disease, and (2) treatment. The associations between the circulating concentrations of mechanistic biomarkers, patient reported outcome measures, and their changes over time, and the primary and secondary outcomes were assessed. Missing data are reported. Significance tests with 2-sided p-values are accompanied by confidence intervals for estimated effect sizes and measures of association. The widths of the confidence intervals have not been adjusted for multiplicity. The p-values for subgroup differences were calculated using the Fisher Exact test and the Kruskal-Wallis test, for categorical and continuous data, respectively. A p-value of 0.05 was taken as statistically significant.
Trial management and timelines
The study was conducted in line with the current Guidelines for Good Clinical Practice in Clinical Trials and STrengthening the Reporting of OBservational studies in Epidemiology guidelines39, and coordinated by a Study Management Group. A Scientific Steering Group had oversight of the study.
Ethics
The study was approved by the UK National Research Ethics Service (Reference 20/NS/0066).
Sources of Funding
This was an investigator-initiated clinical study that was funded by the Chief Scientist Office of the Scottish Government (COV/GLA/Portfolio project number 311300). The funder had no role in the design, conduct (non-voting TSC member), data analysis and interpretation, manuscript writing, or dissemination of the results. C.B, C.D., N.S., R.M.T. were supported by the British Heart Foundation (RE/18/6134217).
The MRI study involved technologies provided by Siemens Healthcare and the National Institutes of Health. HeartFlow (HeartFlow, Redwood City, CA) provided FFRCT. The study was co-sponsored by NHS Greater Glasgow & Clyde Health Board and the University of Glasgow.
Data and code availability
The datasets that support the findings of this study are available from the corresponding author upon reasonable request. Statistical code will be made available by the corresponding author upon reasonable request.
Registration
ClinicalTrials.gov: NCT04403607.
{kind=link}