The results on statin use and its potential benefits for COVID-19 patients are controversial. In a recent meta-analysis, it was reported that “statin use did not improve in-hospital outcomes of COVID-19 infections” [38]; this analysis included 9 studies with a total of 3,449 patients. The results showed that statin use did not improve the outcome severity [OR = 1.64, 95% CI: (0.51–5.23), P = 0.41, I2 = 93%, random-effect modelling] or the mortality rate from COVID-19 infection [OR 0.78, 95% CI: (0.50–1.21), p = 0.26, I2 = 0%, fixed-effect modelling] [38]. This result might be due to their statistical analysis method. In an investigation on the use of statins in chronic renal disease patients with COVID-19, it was shown that statins reduced “the risk of neutrophilia [OR-0.10, 95% CI: (0.01–0.69)]” but did not affect the mortality in these patients [39]. Conversely, a relatively large retrospective study on 13,981 patients with COVID-19 (Hubei Province, China) revealed that statin use decreased all-cause mortality from 9.4–5.2% (a total of 1,219 patients received statins) [14]. In a recent investigation it has been also showed that statin use decreased the in hospital mortality in COVID-19 patients with diabetes [40]. It has also been reported that using statin during hospitalization decrease the chance of ICU admission when compared to non-statin users [41]. It has been also showed that using statin decreased the risk of invasive mechanical ventilation in COVID-19 patients [42]
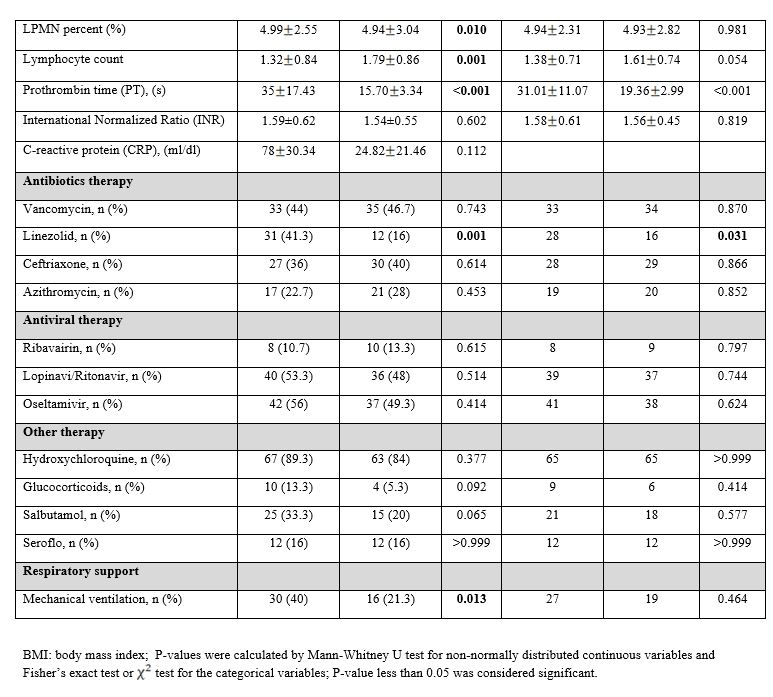
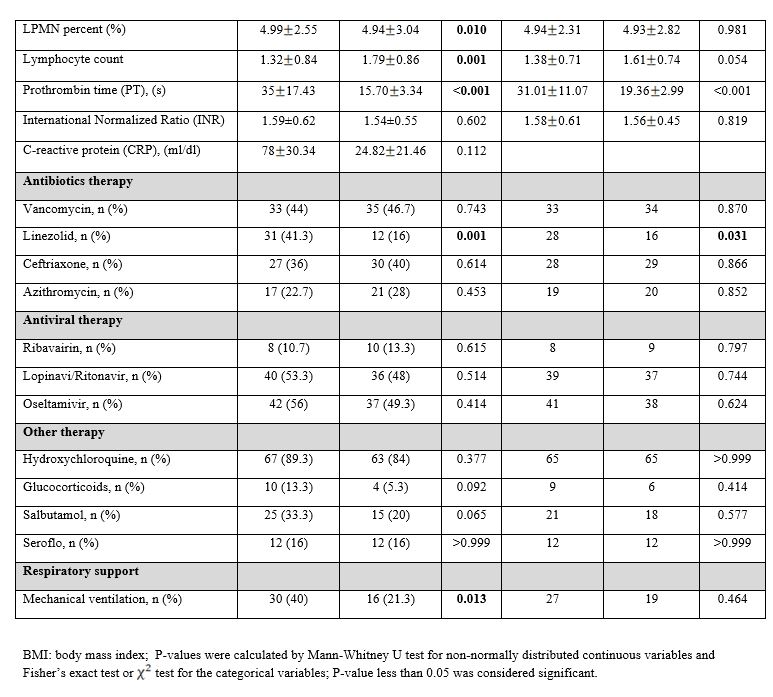
Based on our overall results, we feel that there is an indication that the use of statins may be linked to a lower risk of COVID19 mortality, even though this association did not reach statistical significance [HR = 0.924, 95% CI=(0.205, 4.157), P = 0.918]. In addition, statins significantly reduced the need for mechanical ventilation and improved lung CT in COVID-19 patients. Although promising and clinically relevant, our observed associations between statin use and survival of COVID19 patients were not statistically significant, likely due to impaired power of our analysis as a result of the many patients that had to be excluded, and need to be validated in prospective clinical trials and extensive retrospective studies. Considering the many documented pleotropic effects of statins and the results presented here, we anticipate positive effects of statin use on the clinical outcomes of COVID-19 patients.
Pleiotropic effects of statins have been reported in several malignancies, especially respiratory infections [43, 44], acute lung injury [45], pulmonary hypertension [46], community-acquired pneumonia, chronic obstructive pulmonary disease [47], and interstitial lung disease [48]. Statins have shown various beneficial anti-inflammatory and immunomodulatory properties by affecting intracellular signaling pathways [49, 50] that are independent of their lipid-lowering ability [51]. Furthermore, antiviral effects against the influenza virus have been demonstrated in several in vitro and in vivo studies [52–55]. Statins modulate the antiviral response in human bronchial and epithelial cells, which constitute the first line of defense against invading pathogens [56], and significantly reduce the production of pro-inflammatory cytokines, such as TNF-𝛼 and IL-6, in Crandell feline kidney cells infected with H1N1 [57]. In primary normal human bronchial epithelial cells (NHBE) and human type II pneumocyte cell line A549, simvastatin attenuated viral dsRNA-induced AKT phosphorylation, STAT3 activation, and subsequent production of RANTES [58]. In another study, simvastatin was shown to reduce the replication of H1N1 by blocking RhoA membrane localization, actin filaments condensation, Rab protein expression during endocytosis, and LC3-II protein localization [53].
The effect of statins on the Coronaviridae family is still under-studied. Earlier in 2015, it was proposed that a high dose of atorvastatin may work against MERS-CoV infections by decreasing inflammatory cytokines [59]. However, statins may not be very effective in late-stage patients but timely use of statins could be vital for the survival of MERS-CoV infected patients [59]. Since some investigations had confirmed the association of statin therapy with a reduction in cardiovascular outcomes and mortality in patients infected with influenza, it was also suggested that COVID19 patients, with severe damage to lung tissue caused by a cytokine storm of inflammatory mediators, continue statin therapy for its potential clinical benefit [60]. An in silico docking study highlighted that statins might be efficient inhibitors of the SARS-CoV-2 main protease [61]. Moreover, selective statins (fluvastatin was more efficient than other statins) reduced SARS-CoV-2 cell entry and inhibited infection of human respiratory epithelial cells by either the low pathogenic (coronavirus 229E) or highly pathogenic (2019-nCoV) coronavirus. It was contributed with mild attenuation of SARS-CoV-2 infection in vitro [62]. This study also showed that statin therapy did not cause any additional risk to these patients and that some statins may have a mild beneficial effect on COVID-19 outcome [62].
Autophagy is an important cellular mechanism against different types of stress, including viral infection [3, 63, 64]. SARS-CoV-2 infection likely changes autophagy flux in the infected cells and hijacks it for its replication [3]. The clinical effects of statins described to date have in part been attributed to their impact on the cellular autophagy pathway. Indeed, several studies have reported the involvement of the autophagy pathway as a mechanism for the protective effects of statins in the human lung [65, 66]. Using airway mesenchymal cells, we demonstrated the potential for statins to have beneficial effects in obstructive airways diseases by induction of autophagy via upregulation of p53 [67] as well as through their effects on other pathways, such as the unfolded protein response [68]. Using a mouse model of asthma, simvastatin was shown to ameliorate key asthmatic symptoms (airway remodeling and inflammation) in the lungs via autophagy augmentation [32]. Therefore, it is conceivable that statins may target SARS-CoV-2 infection in lung epithelial cells via the autophagy pathway.
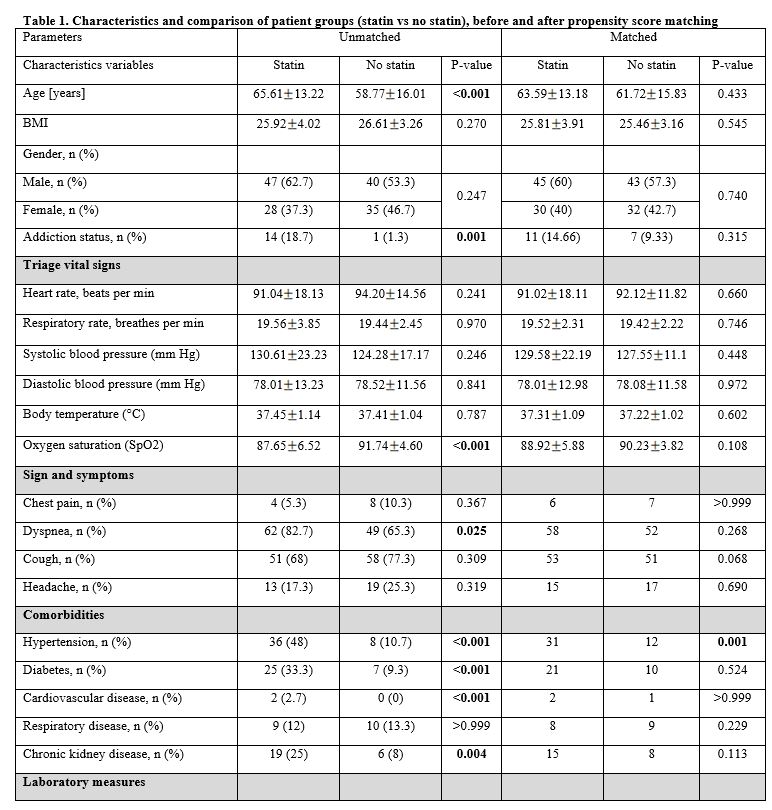
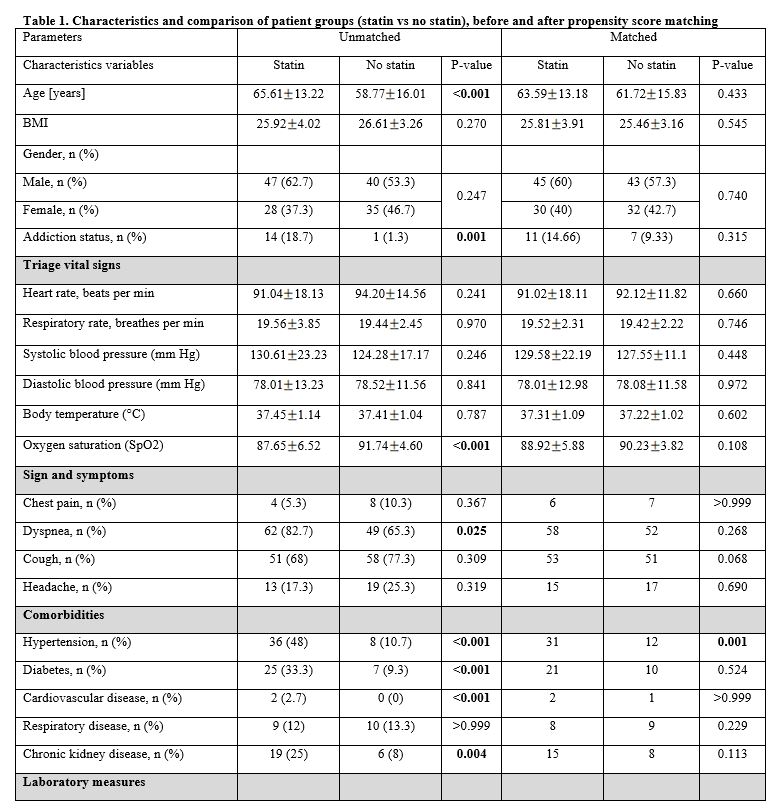
Statins have shown modulatory effects on angiotensin-converting enzyme 2 (ACE2) expression. Qi and co-workers were the first to study the expression of ACE2 in cardio-myocytes of rats with cardiac hypertrophy and reported a decreased expression of both ACE2 mRNA and protein levels in response to 4 weeks of treatment with 5 mg/kg/day of atorvastatin [69]. Later, similar effects on aortic arteries in vascular balloon injured rats treated with the same doses of rosuvastatin for 2 to 4 weeks were reported [70]. However, other studies presented conflicting observations. In a cellular model of vascular smooth muscle cell hypertrophy, atorvastatin recovered the molecular changes induced by TNF-α and increased ACE2 mRNA expression [71]. Using a rabbit model of atherosclerosis, an association between atherosclerosis and a reduced level of ACE2 in both renal and cardiac tissue was established; ACE2 levels were replenished following 3 weeks of atorvastatin administration [72]. Since the significance of ACE2 expression in diabetes surfaced [73], scientists have focused on the potential role of statins in diabetes. Aguilar and colleagues showed that atorvastatin increased ACE2 mRNA in cardiomyocytes of diabetic cardiomyopathic rats, which was associated with a reduction in fibrosis and hypertrophy of the left ventricles [74]. These effects were attributed to the recovered ratio of ACE/ACE2 rather than an increased level of ACE2 [74]. Further studies in diabetic rats confirmed that statin administration increased ACE2 mRNA in cardiac tissue from insulin-controlled groups, although this was not accompanied by significant effects on cardiac fibrosis and reactive oxygen species generation [75, 76]. In our current report, 33% of COVID19 cases that used statins were diabetic. Although diabetes is among the comorbidity factors for COVID-19 mortality, none of the diabetic COVID19 patients on statins enrolled in our study died because of COVID-19 infection.
In addition to their anti-inflammatory actions, our recent investigation showed that statins inhibit tissue damage by reducing extracellular matrix synthesis in airway mesenchymal cells [77, 78]. Several studies have shown beneficial effects of statins in the treatment and recovery of patients with idiopathic pulmonary fibrosis and implied that statins improve lung function by acting on fibrosis mediators [79, 80]. In addition, statins reduce mortality in these patients and those with interstitial lung disease [81]. Simvastatin reduces the connective tissue growth factor and transforming growth factor-beta (TGFβ) in lung fibroblasts through inhibition of Rho signaling [78, 82, 83]. Following a decrease in TGFβ, TGF-β1-induced fibronectin production by fibroblasts and epithelial-mesenchymal transition of respiratory epithelial cells are also reduced [77, 84]. Finally, simvastatin reduces the collagen deposition in alveolar cells of the lung and prevents the progression of pulmonary fibrosis [85].
{kind=link}
{kind=link}
{kind=link}
{kind=link}