Study Design
In this prospective cohort study patients were assessed at 4 time points: ≤ 4 (baseline), 8, 12, and 26 weeks after the onset of acute LBP. At each time point, clinical tests were performed. Patient-reported outcomes were collected using an online survey that queried medical history, demographic variables, LBP-associated pain and the disability level. All participants provided informed consent prior to the start of the examination. The Medical Ethics Committee of the Canton of Zurich, Switzerland (BASEC-no. 2016-02096) approved the study protocol. All experiments were performed in accordance with relevant guidelines and regulations
Participants
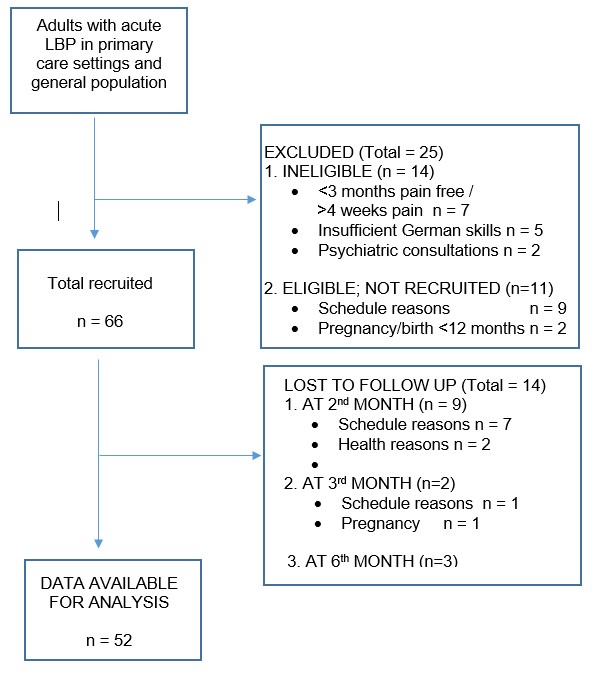
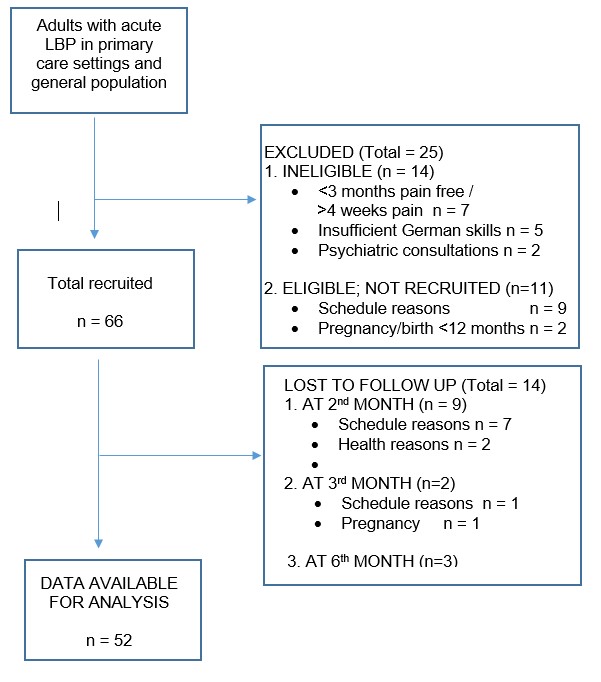
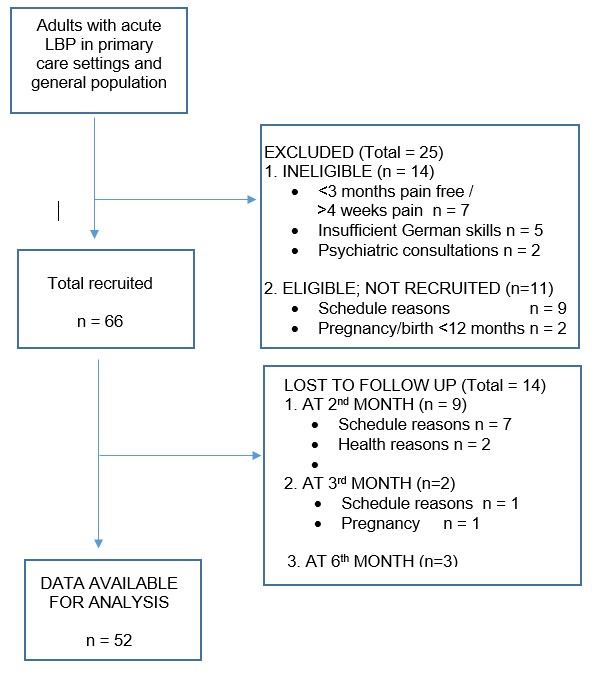
The 66 patients with acute LBP were recruited from private physiotherapy practices, two hospital outpatient practices, and the University Campus using advertisements and mailing lists between December 2017 and October 2018. Inclusion criteria were 1) onset of acute LBP with or without radiation of pain within the last 4 weeks, 2) in case of recurrent LBP: pain-free episode at least 3 months prior to pain onset, 3) age 18–65 years and 4) sufficient German language skills to fill out the questionnaires. The exclusion criteria were: 1) signs of serious pathology, 2) major psychiatric illness necessitating psychiatric/psychological consultations, and 3) current pregnancy or recent birth (past 12 months). Of the 89 candidates screened for eligibility, 66 were enrolled at baseline. Of this group, 86% (n= 57) were available at week 8, 83% (n=55) at week 12, and 79% (n=52) at week 26. The most common reasons for loss-to-follow up were insufficient adherence to the schedule of clinical tests or questionnaire completion and pregnancy (see Figure 1 Supplementary Material). There were no differences between participants and dropouts at baseline.
Patient-reported outcome measures. The online survey was sent as a link by email and the patients were asked to complete the questionnaires within 2 days. Patients who did not complete the questionnaires within this time were sent an electronic reminder, followed by a phone call in case of no response.
Demographic and clinical variables. Baseline sociodemographic data on sex, age, marital status, education level, and number of previous LBP episodes were collected, as well as information on the use of medical services, and sick leave.
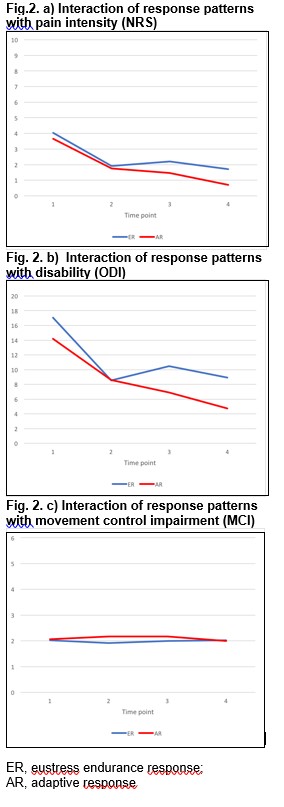
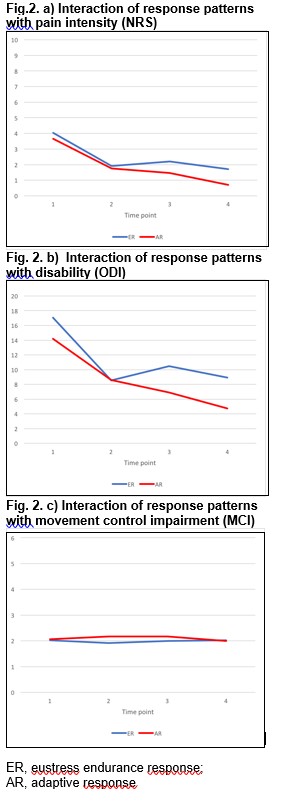
Pain intensity. Present pain, worst pain and average pain intensity of the past week were measured at all four time points using a numeric self-rating scale (NRS) ranging from 0 to 10. The mean pain intensity was then calculated. Areas of referred pain were also documented.
LBP associated disability. The Oswestry Disability Index (ODI) quantifies overall functional disability. The German version of the ODI has excellent test-retest reliability (r = 0.96) and strong correlations with the Roland Morris Disability Questionnaire (r = 0.8) in patients with chronic pain [25].
Depression. The 21-item Depression Anxiety Stress Scale (DASS) questionnaire was designed to assess the severity of depression, anxiety and stress using three subscales [26]. Depression has a cutoff of >10 sum score on the subscale depression, with high internal consistency (Cronbach’s alpha 0.91) and construct validity (r = 0.68) with the Beck Depression Inventory [27].
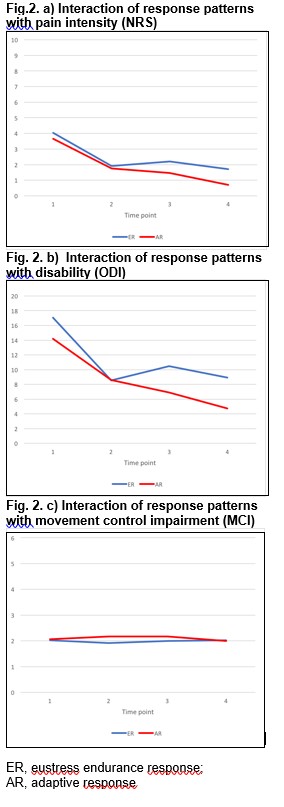
Pain-response patterns. The Avoidance-Endurance Questionnaire (AEQ) was designed to assess pain-response patterns according to four different subgroups: adaptive response (AR), fear-avoidance responses (FAR), distress endurance responses (DER), and eustress-endurance responses (ER) based on the Avoidance-Endurance model [15]. The subgroups were established using the thought suppression scale (TSS) and the behavioral endurance scale (BES), together with the depression subscale of the DASS [28] (S1 Table).
Clinical examination. At each time point, clinical data on pain, MCI, and neurological status (sensory neuron and motor responses) were collected to screen for serious pathology and re-control the exclusion criteria. All investigators underwent a 2-hour training session to ensure the intra- and inter-tester reliability of the clinical tests and study procedure.
Lumbar movement control abilities were evaluated using a battery comprising six active direction-specific movement tests for flexion, extension and rotation. Investigators provided verbal movement instructions and repeated them once in case of incorrect movement execution. Investigators then rated the execution as correct (negative = 0 points) or incorrect (positive = 1 point), with total scores ranging from 0 to 6 and a high score interpreted as high impairment of movement control [29]. The discriminative validity of the test battery in patients with LBP vs. healthy controls was previously demonstrated, with mean scores of 2.2 in patients with LBP and 0.75 in controls (p<0.05) and good to excellent intra- and inter-tester reliability [18,29,30].
Statistical analyses
Descriptive statistics were used to screen for disproportional participant characteristics and data outliers. A 2-way repeated measures analysis of variance (ANOVA) was then conducted with pain-response patterns as the between-subjects factor, time as the within-subjects factor (baseline, 8, 12 and 26 weeks) and pain intensity, disability and MCI as outcome variables. In case of significant time effects, Bonferroni post-hoc tests were applied to determine within-subject differences. Mean values were substituted for missing values. Because age and sex were considered to impact pain, disability and MCI, adjustments were made for their effects using a repeated measure analysis of covariance (ANCOVA). A further adjustment was included for the number of previous LBP episodes (0, 1–2, 3–4, and >4). The relative risk (RR) of pain persistence in each subgroup was examined at 12 and 26 weeks based on two pain categories: < NRS 3/10 and ≥NRS 3/10. Finally, the bivariate correlations of pain intensity, disability, and MCI were calculated using Spearman’s correlations. The significance level was set at p < 0.05. SPSS 25.0 (Statistical Package for the Social Sciences) was used for all statistical analyses.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}