Demographics and clinical presentations
During the study period, a total of 245 patients were admitted for sepsis or septic shock. In the first stage, 6 patients were excluded from the study due to age < 20 years, 4 excluded due to pregnancy, 9 due to leukopenia or hyperleukocytosis, 6 due to hemolysis, and 10 had received albumin or heparin treatment before HBP measurement. A total of 206 patients were initially included, but 21 patients died within 48 hours of admission. Thus, the remaining 185 patients were included for analysis Fig. 1).
We compared the demographic, comorbidity, laboratory results, site of infection, clinical severity, and various outcome variables between survivors and nonsurvivors. Compared to survivors, non-survivors were older, had higher serum levels of procalcitonin and lactate, and had more bloodstream but more pulmonary infection. Nonsurvivors had higher APACHE II or SOFA scores and required mechanical ventilation support more frequently. The comparison of patient characteristics across the two groups is summarized in Table 1.
Table 1
Comparisons of baseline characteristics between survivors and nonsurvivors in patients with severe sepsis and septic shock
| |
Survivors
(N = 137)
|
non-Survivors
(N = 48)
|
P Value
|
|
Demographic characteristics
|
|
|
|
|
Age, mean ± SD, yr.
|
63.21 ± 19.45
|
63.60 ± 17.47
|
0.902
|
|
Female, n (%)
|
48 ± 35.0
|
17 ± 35.4
|
1.000
|
|
Comorbidities, n (%)
|
|
|
|
|
Chronic heart failure
|
13 ( 9.5)
|
5 (10.4)
|
1.000
|
|
Diabetes mellitus
|
31 (22.6)
|
10 (20.8)
|
0.956
|
|
Cerebrovascular disease
|
27 (19.7)
|
8 (16.7)
|
0.803
|
|
Chronic kidney disease
|
19 (13.9)
|
10 (20.8)
|
0.362
|
|
Laboratory results, mean ± SD
|
|
|
|
|
White blood cell count (109/L)
|
13.47 ± 14.36
|
12.58 ± 7.52
|
0.683
|
|
Neutrophil percentage (%)
|
83.81 ± 10.49
|
79.74 ± 20.30
|
0.078
|
|
Procalcitonin(ng/dL)
|
8.06 ± 18.80
|
22.55 ± 31.70
|
< 0.001
|
|
Lactate (mmol/L)
|
2.72 ± 2.64
|
5.51 ± 5.15
|
< 0.001
|
|
Site of sepsis, n (%)
|
|
|
|
|
Bloodstream
|
2 (1.5)
|
6 (12.5)
|
0.005
|
|
Lung
|
112 (81.8)
|
47 (97.9)
|
0.011
|
|
Urinary tract
|
9 (6.6)
|
2 (4.2)
|
0.802
|
|
Abdomen
|
18 (13.1)
|
12 (25.0)
|
0.091
|
|
Soft tissue
|
2 (1.5)
|
1 (2.1)
|
1.000
|
|
Others
|
4 (2.9)
|
1 (2.1)
|
1.000
|
|
Clinical scoring, points, mean ± SD,
|
|
|
|
|
APACHE II score
|
14.58 ± 7.36)
|
23.69 ± 6.43
|
< 0.001
|
|
SOFA score
|
6.47 ± 4.91)
|
13.42 ± 5.60
|
< 0.001
|
|
Number dysfunctional organs, mean ± SD
|
2.7 ± 1.2
|
4.1 ± 1.7
|
0.060
|
|
Organ support, n (%)
|
|
|
|
|
Mechanical ventilation
|
21 (15.3)
|
14 (29.2)
|
0.058
|
|
Renal replacement therapy
|
6 ( 4.4)
|
15 (31.2)
|
< 0.001
|
|
Vasopressor
|
36 (26.3)
|
32 (66.7)
|
< 0.001
|
|
Duration of hospitalization, mean ± SD,days
|
|
|
|
|
Length of ICU stay
|
9.30 ± 9.53
|
10.79 ± 7.93
|
0.334
|
|
Length of hospital stay
|
17.37 ± 12.82
|
11.50 ± 8.38
|
0.004
|
Baseline and dynamic change of HBP among sepsis patients
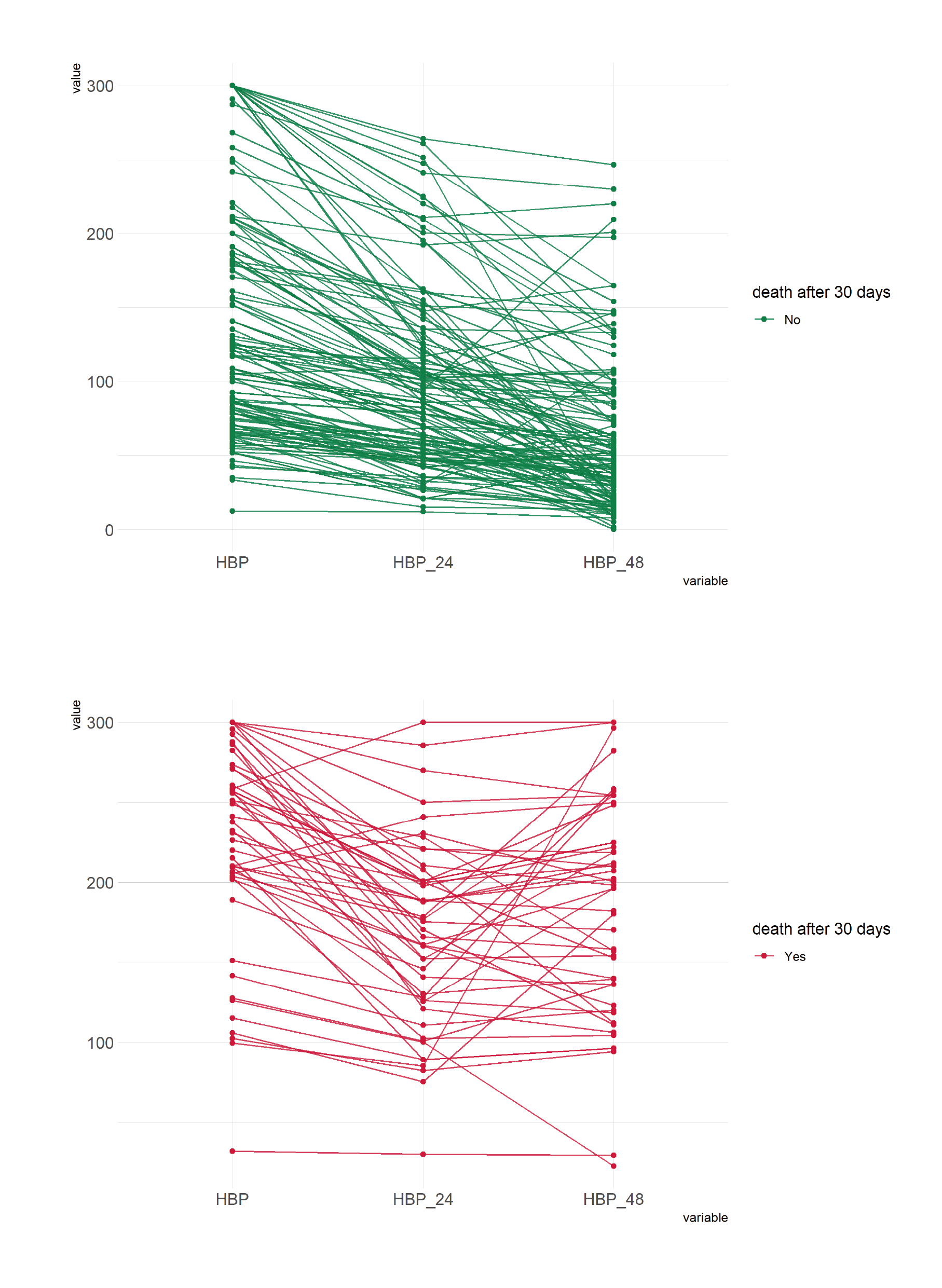
Table 2 compares the baseline and dynamic change of HBP within 48 hours of admission between survivors and nonsurvivors. Mean serum levels of HBP were higher in nonsurvivors at admission, 24 hours and 48 hours. Survivors had significantly higher mean HBP clearance at both 24 hour and 48 hour than nonsurvivors. The time-dependent change of HBP between survivors and nonsurvivors is shown in Fig. 2. At 24 hours, both survivors and nonsurvivors showed a decreasing trend in HBP with nonsurvivors having higher admission HBP levels (Fig. 2A, 2B). At the 48 hours, the decrease was more pronounced in survivors (Fig. 2C) than nonsurvivors. Several nonsurvivors even had higher HBP levels at 48 hours compared to HBP levels at admission (Fig. 2D). The serial measurements of serum level of HBP for each patient is shown in Supplementary Fig. 1.
Table 2
Comparisons of HBP and HBPc dynamic monitoring levels between survivors and nonsurvivors in patients with sepsis or septic shock
|
Variables
|
Survivors
(N = 137)
|
non-Survivors
(N = 48)
|
P Value
|
|
HBP-initial(ng/mL)
median (IQR)
|
117.41 (75.24-185.45)
|
234.95 (203.13-270.96)
|
< 0.001
|
|
HBP-24 h(ng/mL)
median (IQR)
|
85.42 (51.36-119.58)
|
173.02 (125.77–200.70)
|
< 0.001
|
|
HBP-48 h(ng/mL)
median (IQR)
|
47.72 (24.29–86.12)
|
196.21 (129.60-224.76)
|
< 0.001
|
|
HBPc-24 h(%)
median (IQR)
|
-27.93 (-41.51,-17.25)
|
-21.87 (-35.86,-14.16)
|
0.142
|
|
HBPc-48 h(%)
median (IQR)
|
-53.88 (-71.83,-35.65)
|
-15.24 (-38.65,-3.13)
|
< 0.001
|
Comparative accuracy of biomarkers and clinical score
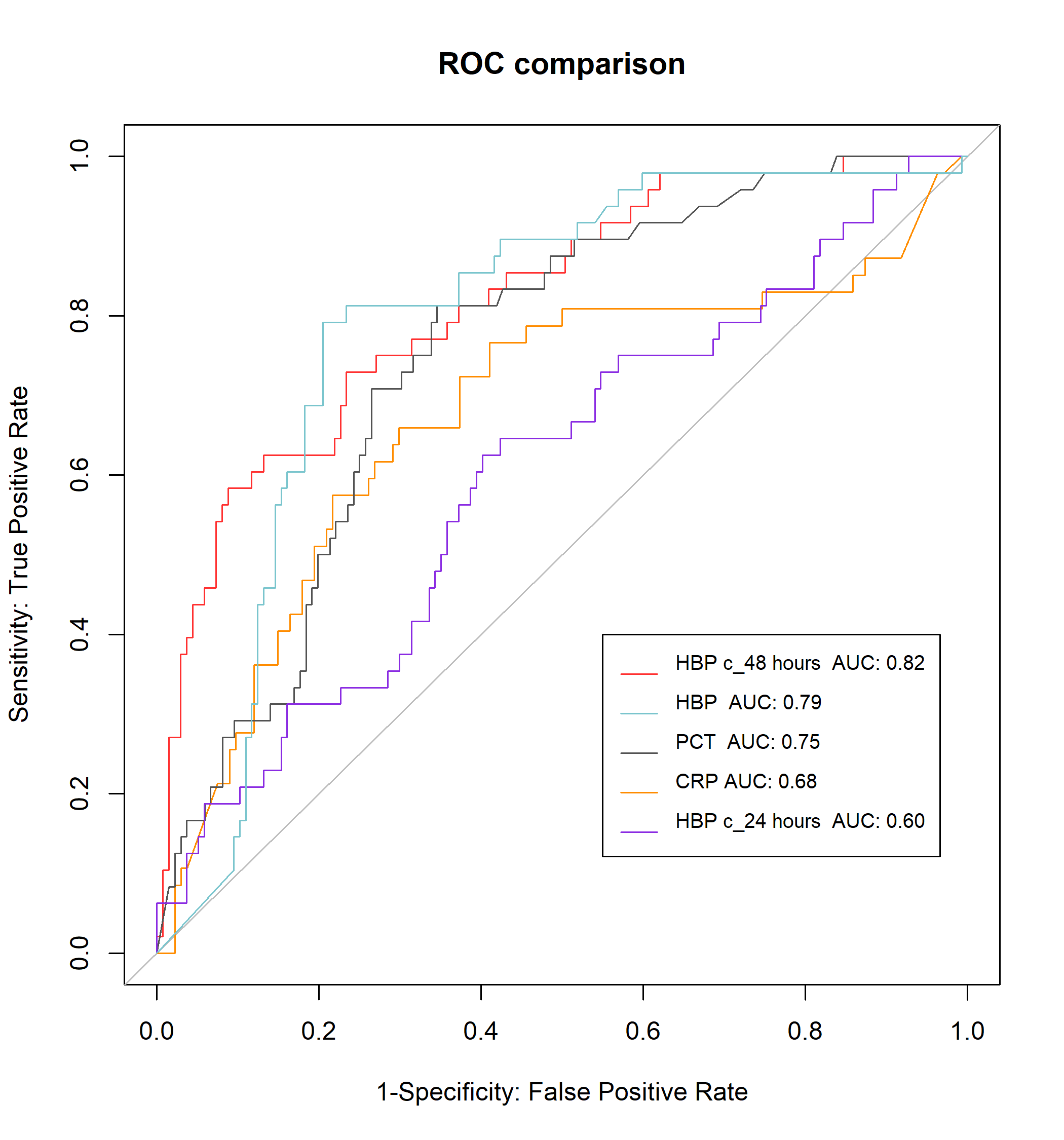
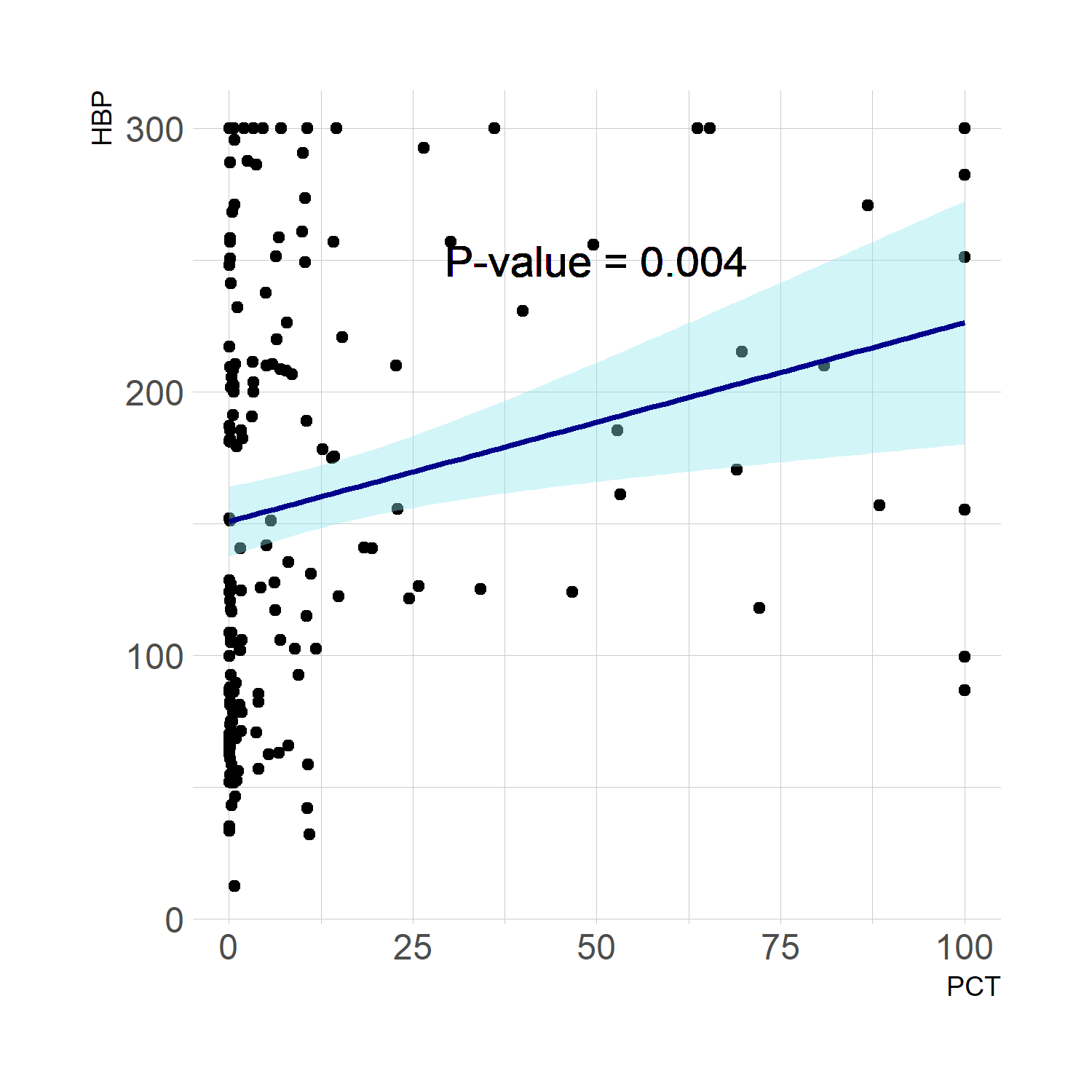
We compared the predictive accuracies of absolute levels and relative changes of various biomarkers. HBPc-48 h had the highest predictive accuracy with an AUC of 0.82, followed by admission HBP (0.79), admission PCT (0.75), admission CRP (0.68) and HBPc-24 h (0.60). Supplementary Fig. 2 shows the ROC curves of each predictive marker. The AUC with 95% confidence intervals, optimal cutoff points, and corresponding sensitivity and specificity are shown in Table 3. At the optimal cutoff of -17.14%, HBPc-48 h can predict 30-day mortality with a sensitivity of 0.58 and a specificity of 0.91. HBP is weakly correlated with PCT concentrations (Spearman correlation 0.21, P = 0.004, Supplemental Fig. 3).
Table 3
Evaluation of the prognosis of severe sepsis and septic shock patients
|
Variables
|
Cut-off level
|
Sensitivity (%)
|
Specificity (%)
|
AUC
|
95%CI
|
|
PCT (ng/dL)
|
1.79
|
0.82
|
0.65
|
0.75
|
0.68, 0.83
|
|
HBP (mg/dL)
|
201.69
|
0.79
|
0.80
|
0.79
|
0.72, 0.86
|
|
CRP
|
91.77
|
0.66
|
0.70
|
0.68
|
0.58, 0.78
|
|
HBPc-24 h (%)
|
-23.26
|
0.63
|
0.60
|
0.60
|
0.51, 0.70
|
|
HBPc-48 h (%)
|
-17.14
|
0.58
|
0.91
|
0.82
|
0.75, 0.89
|
Thereafter, we plotted Kaplan-Meier survival curve at optimal cutoff for baseline HBP (Cutoff: 201.69 ng/mL), HBPc-24 h (Cutoff: -23.26%), and HBPc-48 h (Cutoff: -17.14%) in Fig. 3. In three markers, HBPc-48 h showed the best performance to differentiate survivor and non-survivor groups in 30-day cumulative probability of death (p < 0.0001). For clinical use, we select two cutoff points that can inform clinical decision. Patients who had a HBPc-48 h greater than 50% had a 91.5% survival rate, while patients who had a HBPc-48 h less than 4% had a 86.7% mortality rate.
Lastly, we explored whether or not HBPc-48 h has independent predictive value in addition to common demographic and clinical predictiors. The Cox model showed that HBPc-48 h was independently associated with increased risk of mortality after adjusting for age, gender, shock status, and requirements of mechanical ventilation support. (Table 4)
Table 4
Multivariate binary Cox regression analysis of prognosis in patients with severe sepsis or septic shock
|
Variables
|
HR
|
95%CI
|
P value
|
|
Age > 70
|
1.20
|
0.63,2.29
|
0.575
|
|
Sex (F V.S. M)
|
1.33
|
0.70,2.50
|
0.382
|
|
Shock
|
2.37
|
1.29,4.33
|
0.005
|
|
Mechanical ventilation
|
1.38
|
0.18,10.68
|
0.760
|
|
HBPc-48 h > -17.4%
|
6.34
|
3.46,11.63
|
<0.0001
|
{kind=link}
{kind=link}
{kind=link}