Previous reports have shown a close relationship between R1 resection and OS (or DFS) in PDAC patients [10, 17–19]. Even for patients who underwent PD for PDAC with positive resection margins shown on frozen section, further surgical resection to achieve R0 did not have any significant positive impact on OS [20]. These studies suggested that it is vital to achieve R0 resection on the first attempt of surgical resection. Knowledge on independent risk factors of R1 resection can help surgeons to make better decisions on surgical treatment strategies.
Studies on independent risk factors of R1 resection have been made difficult because of the differences in the definition between the Union for International Cancer Control (UICC) criteria (R1: 0 mm definition) and the UK Royal College of Pathologists (RCPath) criteria (R1: 1 mm definition) [21]. Furthermore, most studies on risk factors of R1 resection did not apply a standard pathological examination protocol, thus making any comparisons among these studies impossible. Also, most studies focused on pancreatectomy did not discriminate between PD and DP. The risk factors of R1 resection in these two different surgical operations for PDAC differ significantly.
With accurate assessment of resection margins by a standardized pathological examination protocol using LEEPP and DWMSIs, and with a single definition of R1 using the 1 mm definition, our study showed marked differences in the R1 resection rates for PD and DP when compared with the published rates of R1 resection [22–26]. In the current study, the rates of R1 resection were similar to the recently reported data for patients who underwent upfront surgery [27]. Previous studies reported R1 resection was frequently present in PV/SMV margins [28] and SMA margins[29], which was closely related to prognosis [30]. Our data also showed similar results in PD. Previous studies who demonstrated lesions in the neck (OR = 5.48) or uncinate process (OR = 2.996) [11], tumor size > 30 mm (OR = 1.13) [12] and grade 3 tumors (OR = 4.05) [28] were independent risk factors of R1 resection. However, there were no studies to clarify independent risk factors separately for R1 in PD and DP. The NCCN guidelines for pancreatic adenocarcinoma recommend operation and resection margins should be assessed separately in PD and DP. Our study supported neck/uncinate tumor, and the N1/2 stage were independent risk factors of R1 resection for PD, and T3 and surgery type were independent risk factors for DP.
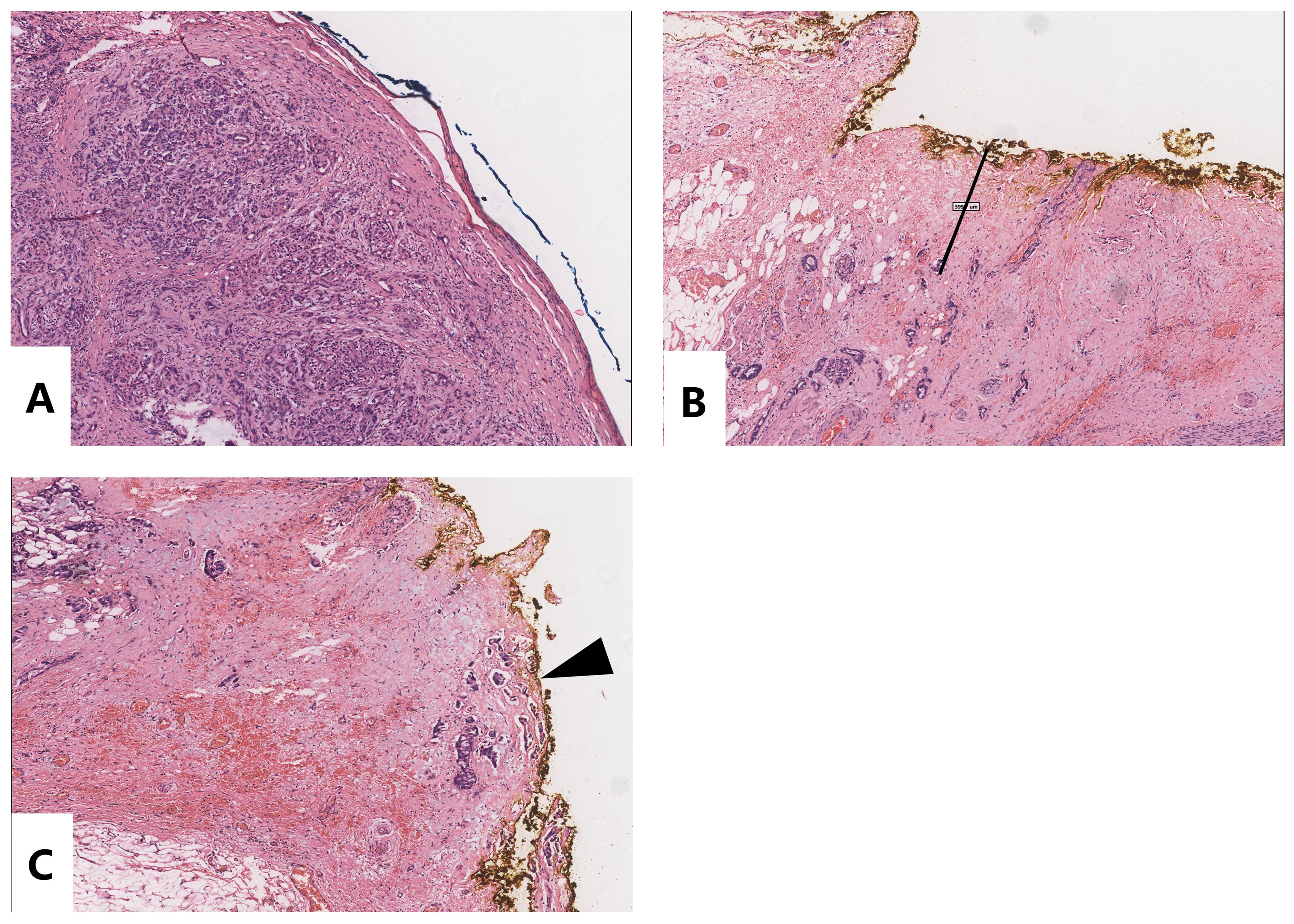
The pancreatic neck is a narrow anatomical region between the pancreatic head and body, lying just anterior to the PV, gastroduodenal artery, and common hepatic artery (CHA) [31]. The uncinate process is closely related to the SMA and the SMV [32]. As a consequence, pancreatic neck or uncinate process cancer are prone to invade these major vessels to become either a borderline or unresectable tumor. R0 resection is technically difficult with involvement of theses vessels. In our study, neck tumor had the highest R1 resection rate, followed by uncinate process tumors. In addition, the most frequently R1 invaded margin in PD (Fig. 3A-F) was the medial margin which included the SMA margin and SMV/PV margin. When the R status of different tumor locations in PD was analyzed (Supplementary Table 1), neck tumors had a significantly higher rate of positive resection margin in the transection margins (38.5%) and medial margins (53.8%). These results suggested that the R0 resection rate of neck tumor was extremely low (3/13 or 23.1%). Our results suggested that surgeons should resect more pancreatic tissues towards the pancreatic tail or even to do TP. To decrease R1 resection in the medial margin, the alternative treatment for patients with pancreatic neck tumor should be neoadjuvant therapy followed by surgery. Supplementary Table 1 also showed that uncinate process tumors had a high frequency (31.8%) of positive medial margins. The regional lymph nodes are mainly distributed along vasculature, and tumor cells can easily invade lymph nodes along the lymphatic drainage pathway. This explain why the N stage is an independent risk factor of R1 resection in PD.
Pancreatic body and tail tumors present late as they do not have symptoms in the early stages [33]. Thus, the pancreatic body and tail tumors are likely to invade beyond the pancreas. Our study suggested that T3 was an independent risk factor of R1 resection.
The present study has several limitations. First, this retrospective study has the intrinsic defects of any retrospective study. Second, the definition of R1 resection margin and the standard procedure for pathological examination of resection margin used in this study made it difficult to compare our results with other published studies. Third, long-term surgical outcomes could not be obtained due to the short study period.
{kind=link}