The present study investigates a large number of risk factors influencing the development of sublingual varices in a very large sample. Until now, only few studies focused the attention on the relation between SV and risk factors such as gender, age, diabetes mellitus, smoking and hypertension in a large population [10, 19], without distinguish the different grade of hypertension. Thus, in our work, beside normotensive subjects, we examined three different hypertension situations, such as new diagnosed, resistant and compensated, clinically identified, excluding subjects presenting either masked hypertension or white coat syndrome [15–18] that could alter the blood pressure evaluation by using the ambulatory measurement along the 24-hour.
Figure 1 shows a significant linear increase of with age in all the four subject groups exhibiting highest occurrence in the range between 70 and 85 years old, confirming the results of [3–6] found on hypertensive patients without distinguishing the clinical grade, suggesting that the arising of SV could be compounded by the aging process. This could be due to the changes in the morphology of connective tissue and blood vessels with age so that SV could be mainly attributed to abnormalities in the circulatory system more present in elderly. However, our findings demonstrate that in the not well controlled hypertensive condition the percentage of subjects presenting SV increases with ageing more than in well controlled hypertension and that in the new diagnosed subjects the increment is less marked than in the other two situations. Therefore, for similar ages, a resistant hypertensive subject is more likely to develop SV than a compensated or a new diagnosed one. A possible explanation is that patients with pharmacologically poorly controlled hypertension show more vascular damage and greater cardiovascular events and that lower levels of vascular disease are present in patients with optimal drug treatment on hypertension and in patients with new diagnosed hypertension [24]. Moreover, normotensive subjects presented a particular peak value in the age group between 70 and 80 years old, possibly due to the presence of some risk factors and to the particular extracted sample.
In addition, the results (Table 2) underlined a relation between SV and either well controlled or resistant hypertension, the latter according to the results of [10, 19] but in contrast with the results of Bhaskar et al. [3], that did not reveal a correlation between SV and 384 subjects presenting resistant hypertension, suggesting that a possible explanation was due to circulatory anastomosis in the venous system of the tongue [3]. The relationship between SV and both compensated and not well controlled hypertension could be related to the presence of hypertension for a greater number of years than in new diagnosed hypertension, producing in both cases vascular damages.
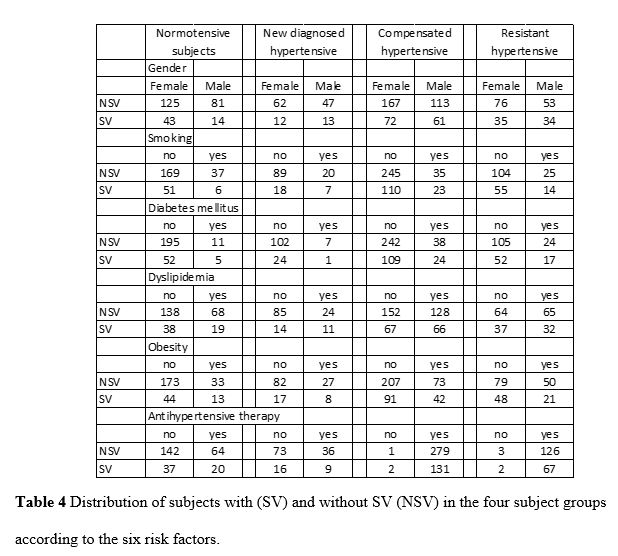
Concerning the relationship between SV and gender, our findings showed (Table 4) that we did not find a significant relation between gender and SV confirming the results of [6, 19], but in contrast with [4] that underlined that female were more likely to have SV, suggesting an hormonal influence on SV. In contrast to the results of another study [6], which found an increase to 58% of SV presence in smokers without hypertension, our results suggested that there was no significant association between smoking and SV in normotensive subjects. This maybe because of the smoking has a preventive effect on the development of varicose veins due to vasoconstrictive effect of nicotine, as suggested by [4, 19]. Analyzing hypertensive subjects, Hedstrom et al [10] underlined an association between the prevalence of SV and non-smokers with hypertension of 44.7% and of SV and smokers with hypertension of 64.7%; we partially confirmed this result founding a significant relationship between smokers and the presence of SV, only for CH group, with lower percentage values (40% and 31%, respectively).
We obtained a significant relationship between SV and dyslipidemia only in subjects with new diagnosed hypertension not yet reported in the literature. However, the relationship seems to be present, albeit non-significantly, even in long-lasting hypertensive patients (compensated), although a greater number of subjects is required to verify this link. Hypertension rarely occurs on its own and often clusters with other cardiovascular risk factors such as dyslipidemia and glucose intolerance producing a multiplicative risk effect.
Furthermore, no association between SV and diabetes mellitus was found, even if [12] underlined that in diabetic subject the most frequent abnormalities were lingual varicosity and that the prevalence of oral abnormalities may be the reflection of the different physiological behaviors of the two clinical types of diabetes. Our results could be justified by the limited number of subjects presenting diabetes. Finally, for the first time in the literature, we found that obesity and antihypertensive therapy showed no relation with the presence of SV, probably a better stratification of obesity would be appropriate.
In order to identify subjects with and without SV, we applied a machine-learning algorithm based on the CART method. By using stepwise regression, only three parameters were identified as input of the algorithm: age, pressure clinical condition and presence of antihypertensive therapy. The resulting tree classifiers (Fig. 3) presented a high SV specificity, i.e. a high probability to predict correctly the absence of SV, a low sensitivity, i.e. a low ability to predict correctly the presence of SV as well as good accuracy (75%) and AUC (67%). The proposed technique demonstrates the powerful capability of some risk factors and of CART technique in differentiating subjects with and without SV. However, despite a good accuracy, the parameters considered are not sufficient to predict with high sensitivity subjects with SV, thus it will be necessary to identify other factors to take into consideration such as hypertension-mediated organ damage indexes, extracted from ECG, echocardiography, echo color-doppler of carotid, CT or MR brain examination.
{kind=link}