Patient characteristics
Patient characteristics are shown in Table 1. Among the 414 patients treated with PEM, 301 were finally enrolled. Their median age was 66 years, and 173 (57.5%) patients were male. Performance status 0/1/2 was seen in 106/159/36 patients, respectively. Stages III and IV were seen in 23 and 199 patients, respectively. Recurrence after definitive treatment (operation or chemoradiation) was seen in the remaining patients (n = 77).
Additionally, we compared PEM-based regimens with another standard regimen during the study period, PTX + CBDCA + Bev, to clarify the PEM-specific predictive response markers [27, 28]. Among the 90 patients treated with PTX + CBDCA + Bev, 80 were enrolled. Age, ECOG-PS, and therapy line of PTX-treated patients were significantly lower than those of PEM-treated patients (P < 0.05).
Table 1
Clinical and demographic features of study subjects
| |
PEM ± Platinum ± Bev
( n = 301)
|
PTX + CBDCA + Bev
( n = 80 )
|
P value
|
|
Age
|
66 [39–92]
|
64 [36–79]
|
0.025 *
|
|
Sex Male/Female
|
172/129
|
54/26
|
0.094
|
|
BMI
|
21.9 [14.6–33.0]
|
22.4 [15.2–30.2]
|
0.137
|
|
Smoking history
|
|
|
|
|
Never/Past/Current
|
106/122/73
|
25/33/22
|
0.754
|
|
Brinkman’s index
|
400 [0-920]
|
400 [0-3600]
|
0.921
|
|
ECOG PS 0/1/2
|
106/159/36
|
40/36/4
|
0.026 *
|
|
Pathological diagnosis
|
|
|
|
|
Adenocarcinoma/Others
|
287/14
|
75/5
|
0.559
|
|
Stage (8th edition)
|
|
|
|
|
ⅢB/ⅢC/ⅣA/ⅣB/Rec/Unknown
|
19/4/110/89/77/2
|
11/2/26/18/23/0
|
0.208
|
|
Driver mutation
|
|
|
|
|
EGFR +/-/Unknown
|
87/200/14
|
27/49/4
|
0.679
|
|
ALK +/-/Unknown
|
15/227/59
|
3/56/21
|
0.410
|
|
Therapy line
|
|
|
|
|
1st line/2nd line/Others
|
179/83/39
|
60/14/6
|
0.038 *
|
|
The data and variabilities are presented as median and range.
Abbreviations: PEM = Pemetrexed, Platinum = Cisplatin or Carboplatin, PTX = Paclitaxel, CBDCA = Carboplatin, Bev = Bevacizumab, BMI = body mass index, ECOG PS = Eastern Cooperative Oncology Group Performance Status, Rec = recurrence after definitive treatment (operation or chemoradiation), EGFR = epidermal growth factor receptor, ALK = anaplastic lymphoma kinase. *: P<0.05 (Unpaired t-test, Chi-square test)
|
Monitoring of leukocyte fractionation during administration of PEM
We examined the transitions of 301 PEM-treated patients in peripheral blood leukocyte fractionation and the NLR at the following PEM administration time points: 1st (pretreatment), 2nd, 4th, 8th, and 16th cycles. ALCs were statistically higher in the long-term administration group throughout the entire treatment period than in the other groups (Figure 2b). There was a small tendency toward lower neutrophil and higher monocyte levels in the long-term administration group, but the difference was not statistically significant (Figure 2a, c). However, NLR was significantly higher in the short-term administration group throughout the entire treatment period compared to the long-term administration group (Figure 2d). Otherwise, transitions of leukocyte fractionation of the PTX-based regimen were not significantly different in the three groups, except for neutrophil at the time point of 2nd cycle (Figure 2e-h). To examine the independent factors of long-term PEM response, we additionally performed multiple logistic regression analysis. Age, sex, performance status, smoking history, stage according to 8th edition of the TNM classification, line of therapy, platinum combination, blood cell counts, and NLR were used as variables. Age, stage, ALC, and NLR were significantly related to the long-term PEM response in the univariate analysis (p<0.05). Age, stage, and blood cell counts were identified as independent factors related to the long-term PEM response in the multivariate analysis (Table 2).
Table 2
Logistic regression analysis for prognostic factors of long-term (≧17 courses) response of pemetrexed
|
|
Univariate analysis
|
Multivariate analysis
|
|
Characteristics
|
P value
|
Hazard ratio
(95%CI)
|
P value
|
Hazard ratio
(95%CI)
|
|
Age
|
0.006 *
|
1.067 (1.018-1.118)
|
0.027 *
|
1.068 (1.007-1.132)
|
|
Sex
|
0.588
|
0.797 (0.351-1.810)
|
0.125
|
0.413 (0.133-1.279)
|
|
ECOG PS
|
0.228
|
3.485 (0.457-26.580)
|
0.459
|
0.441 (0.051-3.851)
|
|
Smoking history
|
0.425
|
0.691 (0.279-1.713)
|
0.261
|
0.492 (0.143-1.694)
|
|
Stage (8th edition)
|
0.013 *
|
0.656 (0.470-0.914)
|
0.030 *
|
0.666 (0.461-0.962)
|
|
Therapy line
|
0.630
|
1.232 (0.526-2.887)
|
0.876
|
0.918 (0.313-2.690)
|
|
Platinum combination
|
0.463
|
1.378 (0.585-3.247)
|
0.764
|
0.841 (0.272-2.604)
|
|
Neutrophils(/㎟)
|
0.228
|
1.000 (1.000-1.000)
|
0.041 *
|
1.000 (0.999-1.000)
|
|
Lymphocytes(/㎟)
|
0.020 *
|
1.000 (1.000-1.001)
|
0.033 *
|
1.001 (1.000-1.001)
|
|
Monocytes(/㎟)
|
0.337
|
1.001 (0.999-1.003)
|
0.016 *
|
1.001 (1.001-1.007)
|
|
NLR
|
0.023 *
|
0.693 (0.505-0.951)
|
※
|
※
|
|
Abbreviations: ALC = absolute lymphocyte count (/mm3), ECOG PS = Eastern Cooperative Oncology Group Performance Status, NLR = Neutrophil-to-Lymphocyte ratio, 95%CI = 95% confidence interval. *: P<0.05 (Binomial logistic regression)
※: Not available due to multi-collinearity.
|
Association of leukocyte fractionation with clinical outcomes in PEM-based regimens
We tested whether the pretreatment ALC could serve as a sensitive and specific predictive biomarker for PEM combination therapy compared to other standard combination therapies in a clinical setting. Of the 301 patients, 211 patients who received the PEM+platinum±Bev regimen were enrolled in the analysis and classified into one of the following three groups: high ALC (ALC≥2000), intermediate ALC (2000>ALC≥1000), and low ALC (ALC<1000) with the median PFS as 4.9, 5.2, and 3.4 months, respectively. The median PFS was statistically longer in the high ALC group (P=0.010, HR: 0.496, 95% CI: 0.296–0.829) and the intermediate ALC group (P=0.024, HR: 0.672, 95% CI: 0.474–0.952) in patients on the PEM+platinum±Bev regimen (Figure 3a).
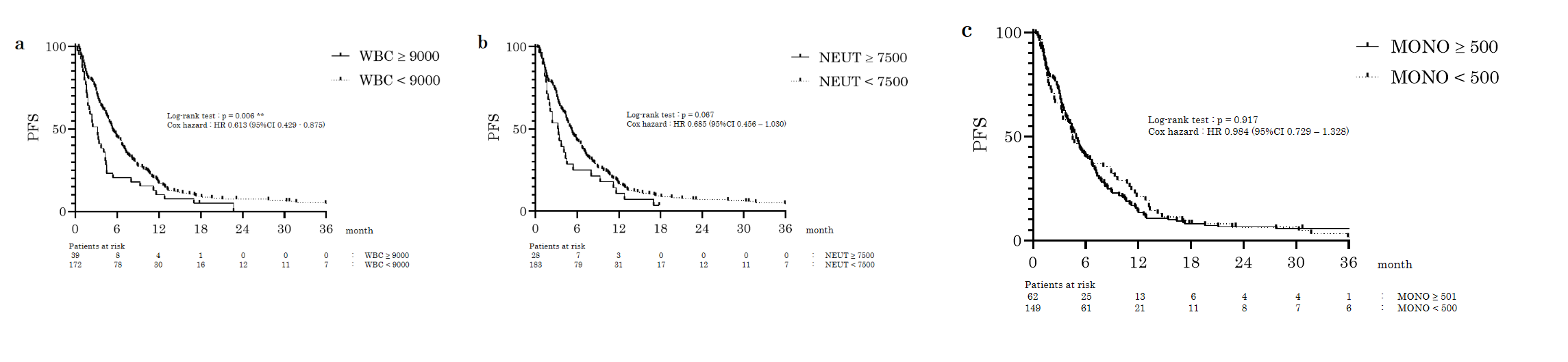
We enrolled 117 PEM-treated patients who were receiving 1st line treatment and were driver mutation negative for OS analysis. The median OS was 16.8, 21.9, and 12.2 months, respectively, and tended to be longer in the high ALC group (P=0.065, HR: 0.500, 95% CI: 0.244–1.027), and was significantly longer in the intermediate ALC group (P=0.012, HR: 0.517, 95% CI: 0.308–0.866) in patients treated with the PEM+platinum±Bev regimen (Figure 3c). For comparison, the 80 patients who received PTX+CBDCA+Bev were analyzed among the three groups (high, intermediate, and low ALC groups). The median PFS was 4.9, 5.2, and 3.4 months, respectively (Figure 3b). Among the 47 patients treated with 1st line therapy who were driver mutation negative, the median OS was 12.6, 25.1, and 15.3 months, respectively. There were no statistically significant differences between any of the groups in the PTX+CBDCA+Bev regimen (Figure 3d). High white blood cell (WBC) and neutrophil counts before treatment tended to be associated with a worse prognosis. The median PFS in the high and low WBC groups were 3.2 and 5.3 months, respectively, and were statistically longer in the high WBC group (P=0.006, HR: 0.613, 95% CI: 0.429–0.875) in patients who received the PEM+platinum±Bev regimen (Supplementary Figure 1a). The median PFS in patients with high and low total neutrophil counts was 3.3 and 5.2 months, respectively, and the patients with a high neutrophil count group showed a tendency towards a longer PFS, although the difference was not statistically significant (P=0.067, HR: 0.685, 95% CI: 0.456–1.030; Supplementary Figure 1b). There were no statistically significant differences in monocyte counts (Supplement Figure 1c).
Association of NLR with clinical outcomes in PEM-based regimens
Similarly, we verified whether the NLR accurately reflects the therapeutic effects of chemotherapy. We recruited 211 patients who received PEM+platinum±Bev with the same criteria as in the ALC analyses and divided them into two groups: high NLR group (NLR≥3.00) and low NLR group (NLR<3.00). The median PFS (months) was 3.8 and 5.8, respectively, and the low NLR group had a significantly longer PFS (P=0.026, HR: 0.725, 95% CI 0.547–0.962; Figure 4a). Among the 117 patients who were receiving treatment as 1st line therapy and who were driver mutation negative, the median OS was 14.3 and 29.7 months, respectively, and the median OS was significantly longer in the low NLR group (P=0.015, HR: 0.588, 95% CI: 0.384–0.900; Figure 4c).
Otherwise, for the 80 patients who received PTX+CBDCA+Bev, the median PFS was 6.3 months (high NLR group) and 7.8 months (low NLR group), with no statistically significant difference (p=0.456; Figure 4b). Among the 47 patients treated with 1st line therapy who were driver mutation negative, the median OS in the low and high NLR groups were 14.1 and 20.8, respectively, with no statistically significant difference (p=0.152; Figure 4d).
PD-L1 expression levels in tumor tissues in the long-term PEM administration group
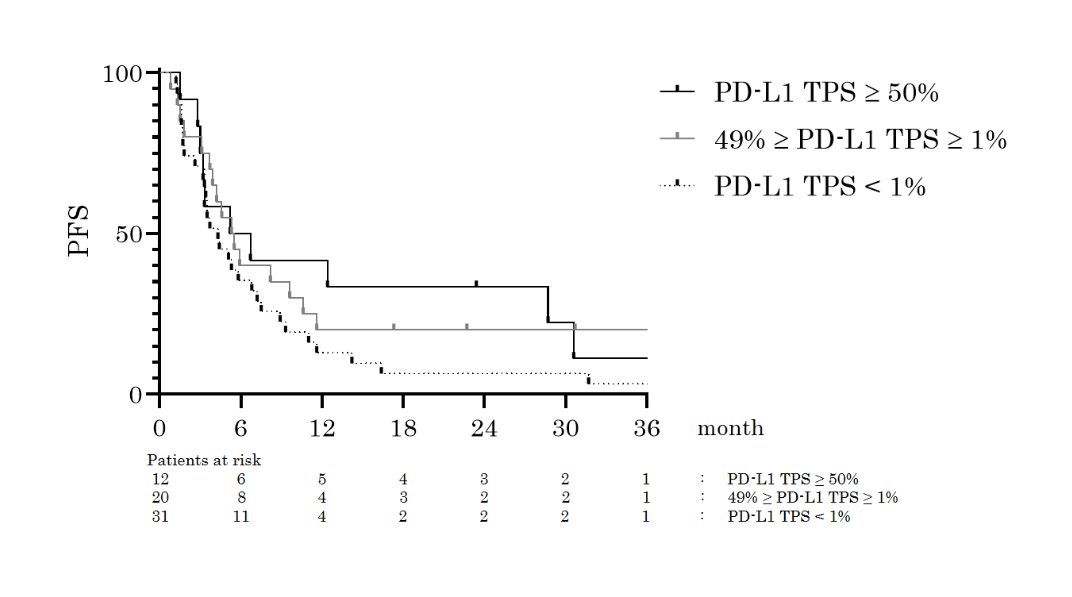
We measured the percentage of PD-L1 expression in tumor tissues from 63 patients treated with PEM+platinum±Bev by bronchoscopic biopsy or pneumonectomy. They were categorized according to the following three groups: high PD-L1 expression (PD-L1 TPS≥50%), low PD-L1 expression (49%≥PD-L1 TPS≥1%) and no PD-L1 expression (PD-L1 TPS<1%). The relationship between the number of PEM treatment cycles and PD-L1 expression levels was then analyzed. The number of PEM treatment cycles was significantly higher in the high PD-L1 expression group than in the no PD-L1 expression group (P=0.031; Figure 5). The Kaplan–Meier curves showed a trend toward better PFS in the higher PD-L1 expression group, but the difference was not statistically significant (Supplement Figure 2).
Measurement of PD-1 lymphocytes in the long-term PEM administration group
We measured PD-1 expression in the peripheral blood lymphocytes of patients who had undergone long-term administration (n=5) or intermediate/short-term administration (n=5) of PEM. An additional five chemo-naïve patients were also included as a control group. The mean levels of PD-1 expression in the peripheral blood lymphocytes were significantly higher in the long-term PEM group than in the intermediate/short-term PEM group (P=0.036; Figure 6).
Effect of preceding PEM on ICI treatment
To determine the effect of previous PEM treatment on immunotherapy outcomes, we analyzed 82 patients who received ICIs after undergoing PEM-related regimens. PFS was not significantly different regardless of previous PEM treatment cycles (Table 3). However, the frequency of immune-related adverse events (any grades) was significantly higher in the group who had undergone long-term administration of PEM compared to the other groups (45.5% vs. 18.3%, P=0.043; Table 4).
Table 3
Treatment effect of immune checkpoint inhibitors after pemetrexed treatment failure
|
Efficacy
|
Long-term
administration
( n = 11 )
|
Intermediate-term
administration
( n = 16 )
|
Short-term
administration
( n = 55 )
|
|
Cycles
|
6.1±8.5
|
5.6±3.2
|
6.2±8.3
|
|
PFS (month)
|
5.5±6.9
|
3.8±2.7
|
3.4±4.4
|
|
Data are presented as mean±SD.
Abbreviations: PFS = progression free survival
|
Table 4
Adverse effects (any grades) of immune checkpoint inhibitors after pemetrexed treatment failure.
|
Adverse effects
|
Long-term
administration
( n = 11 )
|
Intermediate-term
administration
( n = 16 )
|
Short-term
administration
( n = 55 )
|
|
irAE
|
5 (45.5%) *
|
3 (18.8%)
|
10 (18.2%)
|
|
ILD
|
4 (36.3%)
|
2 (12.5%)
|
2 (3.6%)
|
|
Others
|
1 (9.1%)
|
1 (6.3%)
|
9 (16.4%)
|
|
Abbreviations: irAE = immune-related adverse events; ILD = interstitial lung disease
*: P<0.05 (Chi-square test)
|
{kind=link}
{kind=link}