Baseline characteristics
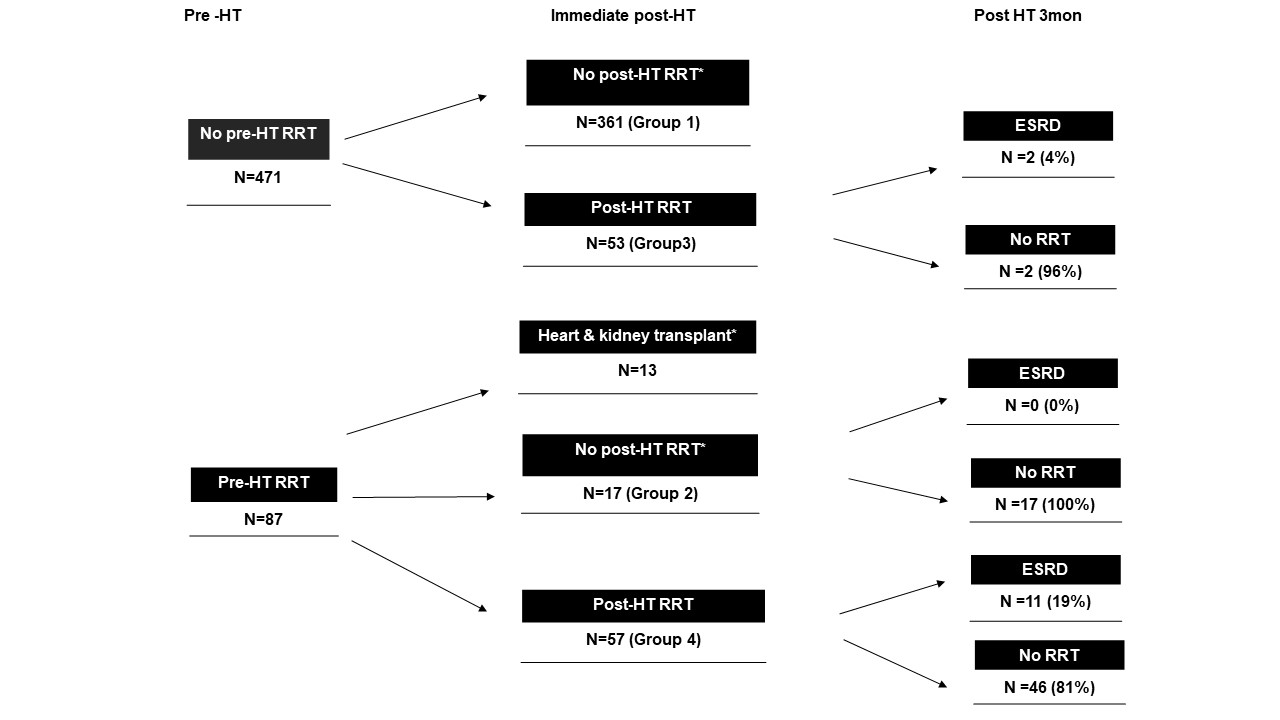
The median follow-up was 22 months (9–39 months). Among the 501 patients, 13 underwent combined HKTx; all of these patients were on dialysis preoperatively. Among the 488 patients who underwent isolated HTx, 74 were on either continuous renal replacement therapy (CRRT) (n=62) or conventional hemodialysis (HD) (n=12) before HTx (groups 2 and 4).
Table 1 shows the baseline characteristics of patients who underwent isolated HTx in relation to perioperative RRT status. Patients from group 1 had longest waiting list duration, while patients in group 2 and 4 had relatively short waiting list duration, suggesting patients in group 2 and 4 are likely to be more rapidly decompensated HF patients. Group 4 included more patients with ischemic heart disease and fewer patients with idiopathic dilated CMP than did the other groups. Patients who needed preoperative RRT (groups 2 and 4) were more likely to have diabetes mellitus (DM) compared to patients in the other groups, although this difference was not statistically significant. Patients who needed preoperative RRT (groups 2 and 4) were also more likely to need pre-HTx mechanical cardiac support (p <0.001) and pre-HTx mechanical ventilator (p <0.001) than patients in the other groups. Mean preoperative BUN and creatinine values were significantly higher in group 4 than in the other groups.
Clinical outcome
Postoperative clinical characteristics of 4 groups are described in supplementary table 1. Significantly more patients from group 4 experienced primary graft failure. Right ventricular systolic pressure were higher in patients who were supported with postoperative RRT (group 3 and 4) at 1 month after HTx.
After HTx, more patients in group 4 had dialysis-dependent ESRD (p < 0.001) than patients in the other groups (Figure 1). During the first 6 months of follow-up, most patients from group 4 developed dialysis-dependent ESRD. After the first 6 months, patient status in relation to dialysis-dependent ESRD stabilized. Among the patients who needed early post-HTx RRT (groups 2 and 4), those from group 2 were less likely to have dialysis-dependent ESRD (11.8%) than those from group 4 (36.8%, p = 0.013). A summary of renal outcome is described in supplementary Figure 1.
Table 2 shows the renal function of all patients who underwent isolated HTx at 6 months and 12 months post-HTx. BUN and creatinine levels were significantly higher in group 4 than in the other groups at both 6 months and 12 months post-HTx. None of patients who became dialysis dependent ESRD recovered to be dialysis free.
Table 3 shows univariate and multivariable analyses for progression to dialysis dependent ESRD after HTx. From multivariable analysis, insulin dependent DM and postoperative RRT were significantly associated with progression to ESRD after HTx. Preoperative RRT did not remain to be statistically significant after adjustment of other variables. Supplement table 2 show subgroup analysis to predict progression to ESRD after HTx according to preoperative RRT status. The significant clinical predictors for progression to ESRD differed between two subgroups. In a preoperative RRT (-) subgroup, the needs for preopertive mechanical ventilation, preoperative mechanical cardiac support, baseline eGFR, baseline creatinine, postoperative RRT, and primary graft failure were significant clinical factors in univariate analysis. However, in a preoperative RRT (+) subgroup, insulin dependent DM and early postoperative RRT were significant clinical predictors.
Univariate analysis showed that insulin-dependent DM, preoperative mechanical ventilation, preoperative mechanical cardiac support, preoperative RRT, preoperative eGFR, preoperative creatinine, cardiopulmonary bypass time, early postoperative RRT and primary graft failure were associated with post-HTx ESRD. However, after adjusting for confounding variables, insulin-dependent DM, and early postoperative RRT were the only variables that were independently associated with post-HTx dialysis-dependent ESRD.
All-cause mortality after HTx
After HTx, patients in group 4 had significantly higher mortality than patients in the other groups (4-year survival rate = 51.9%) (Figure 2). Patients who underwent combined HKTx showed comparable survival (4-year survival rate = 92.3%) to patients in group 1 (4-year survival rate = 90.3%). Patients in group 2 also showed comparable survival to those in group 1 (4-year survival rate =: 94.1%). Univariate analysis revealed that preoperative DM, preoperative mechanical ventilation, preoperative mechanical cardiac support, preoperative RRT, and early postoperative RRT were significant independent predictors of all-cause post-HTx mortality (Table 3). However, preoperative eGFR and preoperative creatinine levels were not associated with all-cause mortality after HTx (Table 3). In multivariate analysis, preoperative DM and early postoperative RRT were the only independent predictors of all-cause mortality after HTx.
Table 4 summarizes the univariate and multivariate analyses for all-cause mortality after HTx. From multivariable analysis, postoperative RRT and primary graft failure the significant predictors of all-cause mortality after HTx. Supplement table 3 shows subgroup analysis according to preoperative RRT status. In preoperative RRT (-) group, from univariable analysis, early postoperative RRT, ESRD progression after HTx, and primary graft failure were statistically significant clinical predictors of all-cause mortality after HTx. From multivariate analysis, early postoperative RRT was the only significant clinical factor. In preoperative RRT (+) group, early postoperative RRT and primary graft failure were significant predictors for mortality after HTx from multivariate analysis.
{kind=link}