In the present study, we first investigated 65 circulating inflammatory biomarkers simultaneously in AIS patients and their relationship with long-term neurological outcomes. We found that plasma HGF and sIL-2R were each independently associated with increased risk of unfavorable outcomes at 3 months after AIS in our study. Furthermore, adding plasma HGF or sIL-2R to traditional risk factors could improve the risk stratification for unfavorable outcomes. And adding HGF and sIL-2R simultaneously to the basic model offered the greatest incremental predictive capacity for the primary outcome. These findings indicated that increased plasma HGF and sIL-2R were associated with unfavorable prognosis of AIS and might be potential prognostic biomarkers for AIS.
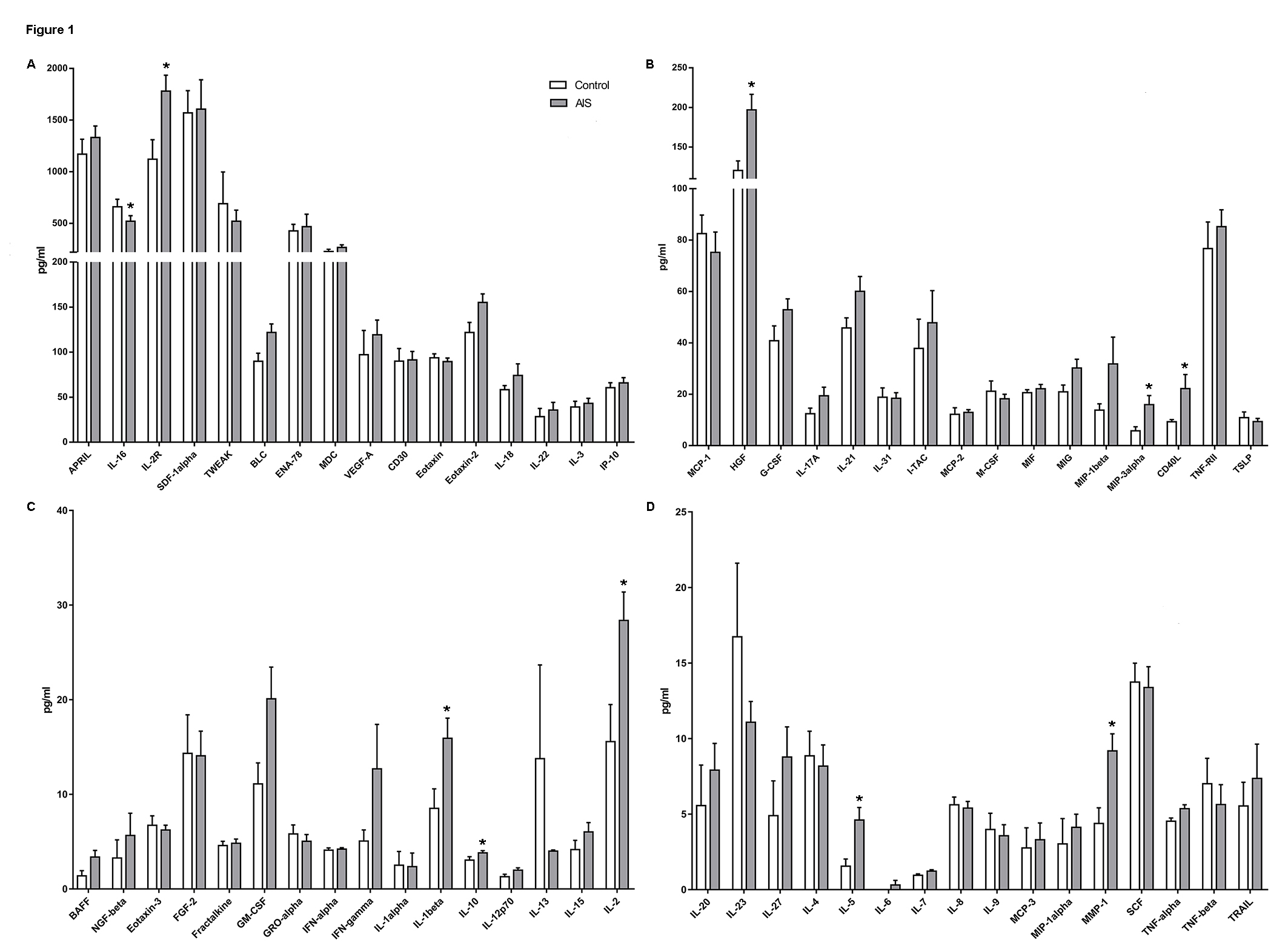
Inflammation is involved in the pathological process of ischemic stroke. Few studies have globally investigated the alterations of inflammatory cytokines in AIS patients and healthy controls. We first screened 65 inflammatory cytokines in our patient cohort by Immune Monitoring 65-Plex Human ProcartaPlex Panel. Ten cytokines (HGF, IL-1β, IL-2, sIL-2R, IL-5, IL-10, IL-16, MIP-3α, CD40L and MMP1) were screened to change significantly (Supplementary Figure 1). Then we collected plasma from in 204 acute ischemic stroke (AIS) patients and 76 healthy controls, and found that seven cytokines including HGF, IL-1β, IL-2, sIL-2R, IL-5, IL-10, and MIP-3α indeed upregulated and had diagnostic capacity in AIS patients. Therefore, our first contribution was to identify two new biomarkers sIL-2R and MIP-3α, which can provide references to other studies and help target particular pathways to prevent the progression of ischemic stroke.
Then, in the univariate analyses, higher plasma HGF, sIL-2R and IL-16 levels were found to be associated with increased risk of unfavorable outcomes, while higher IL-2, and IL-1β levels were associated with decreased risk of unfavorable outcomes. Next, after adjusting for potential risk factors in binominal multivariate analysis, HGF and sIL-2R remained associated with increased risk of unfavorable outcomes, suggesting that plasma HGF and sIL-2R at baseline may be potential predictive biomarkers for prognosis of AIS. Furthermore, the addition of plasma HGF, sIL-2R or both to conventional risk factors was shown to improve risk predictions for the primary outcome. Therefore, this is the first research showed that plasma sIL-2R might be useful in risk stratification in AIS prognosis and could be beneficial for the selection of high-risk patients who should receive aggressive monitoring and therapeutic interventions in future clinical practice.
In recent years, serum HGF has emerged as a novel biomarker for cardiovascular and cerebrovascular diseases. Bielinski et al[19] reported that HGF is a biomarker of atherosclerotic disease and is associated with subclinical and incident coronary heart disease. Moreover, Susen et al[20] found that high serum HGF is an independent predictor of a composite of death and myocardial infarction. In terms of stroke, HGF was proved to be positively associated with the incidence of stroke[21, 22], and Zhu et al[23] reported that higher HGF was associated with mortality but not disability at 3 months after ischemic stroke onset. However, Zhu et al included patients within 48 hours of symptom onset and excluded patients treated with rt-PA. By comparison, patients’ blood in our study was collected within 24 hours before they received any treatment. Thus, the level of HGF in our study could reflect more about the authentic pathological change of AIS without the influence of other factors. Next, we included patients who received rt-PA therapy. rt-PA therapy is a widely accepted treatment strategy for AIS patients within 4.5 hours after symptom onset and can reduce patients’ disability to a large extent[24]. Hence, most patients will accept rt-PA treatment if their onset time is less than 4.5 hours, and including patients with rt-PA therapy could better fit real clinical settings. Moreover, Zhu’s study only ruled out AIS patients in deep coma, without considering patients whose premorbid mRS ≥ 2. However, for patients with a severe disability, they had a higher probability of having a poor prognosis, which may result in statistical bias. Therefore, we only included patients whose premorbid mRS ≤ 1 minimize this bias. The mechanism of HGF was clarified in the basic research. HGF is a pleiotropic cytokine that can regulate different cellular functions in developmental and pathological situations. According to prior studies, HGF can enhance the proliferation of neural precursor cells and increase neuronal differentiation, thus protecting against ischemic stroke[25]. The other underlying mechanisms might include promoting the migration of immune cells and secretion of pro-inflammatory chemokines[26] and accelerating the progression of atherosclerotic lesions[27], thus increasing the risk of unfavorable prognosis.
Moreover, we first reported that sIL-2R was independently associated with increased risk of unfavorable outcomes in AIS. It can be seen in our data that sIL-2R is a high abundance protein in plasma. Therefore, it is easy to detect and suitable as a molecular marker. SIL-2R, a membrane receptor for IL-2, is expressed on the surface of activated T-cells and is shed into the circulation in a soluble form as sIL-2R. Previous research indicated that elevated serum levels of sIL-2R were associated with a poor prognosis in autoimmune diseases, such as multiple sclerosis and follicular lymphoma[28]. Peter et al reported that sIL-2R was positively associated with internal carotid wall thickness, cardiovascular disease mortality, incident cardiovascular disease and stroke[29]. In addition, sIL-2R was significantly higher in ischemic left ventricular dysfunction patients[30] and was associated with a worse prognosis for dilated cardiomyopathy patients[31]. Similarly, we first found that sIL-2R was positively associated with poor functional outcomes in AIS patients. We speculate that abnormal expression of sIL-2R is associated with the aberrant activation of T cells and promotion of neuroinflammation after ischemic stroke[32]. Importantly, according to our supplementary data (Tables 1 and 2), the number of neutrophils in the HGF high expression group was higher than that in the low HGF expression group, while the number of lymphocytes in the high sIL-2R expression group was lower than that in the low sIL-2R expression group. And previous studies suggested that high levels of neutrophils and low levels of lymphocytes were both associated with poor functional outcomes after AIS[33]. Above all, it is of interest to further elucidate the precise mechanisms between increased sIL-2R levels and unfavorable prognosis of AIS.
However, there are some limitations in our study. First, our study lacked data on infarct volume in MRI or CT scan. Patients who met the criterion of intravenous therapy should receive CT scans to exclude cerebral hemorrhage and should be infused with thrombolysis drugs as early as possible[34]. So nearly half of the patients in our study did not have a premorbid MRI scan. Besides, infarcts are not obvious and stable on early CT scans, and the severity of neurological dysfunction is not always proportional to the size of infarct volume; hence, it was reasonable that we did not include infarct volume in our study. Second, our study was performed mainly in Chinese individuals, and the patient sample was somewhat small, limiting the generalizability of the results to other ethnicities. Further studies with larger sample sizes are needed to verify our findings.
{kind=link}