Concise and accurate prognostic prediction models for patients with malignancy are essential for clinical decision-making and scientific research. Indeed, TNM stage is the most widely used survival predictor for cancer patients. However, identifying more prognostic factors and a more individualized model will certainly improve the accuracy of clinical outcome prediction. In this study, we used the SEER database, a large-scale population-based cancer registry program, to explore the clinical characteristics of 4087 patients with LPA and identified the factors associated with distant and lymph node metastases in LPA patients. After that, we developed and validated accurate and personalized prognostic nomograms predicting the 1- and 5-year OS and CSS of patients with LPA.
The survival outcomes of LPA patients with poor prognostic factors were undesirable, and the median OS of advanced LPA patients was 20.1 months (9). However, the prognosis of advanced LPA patients could be improved by appropriate treatments, including chemotherapy and EGFR tyrosine kinase inhibitors (TKIs) (9). The 5-year disease-free survival of LPA patients after complete surgical resection was approximately 90% (10). With the evaluation of the nomograms generated in our study, more aggressive treatments are recommended for high-risk patients with LPA, and appropriate shortening of the follow-up interval is encouraged to detect the occurrence of endpoint events as early as possible. For example, older, unmarried, black men with sizeable tumors and advanced TNM stages are recommended for frequent follow-up and more aggressive treatments, including primary tumor resection, when they meet the operational criteria.
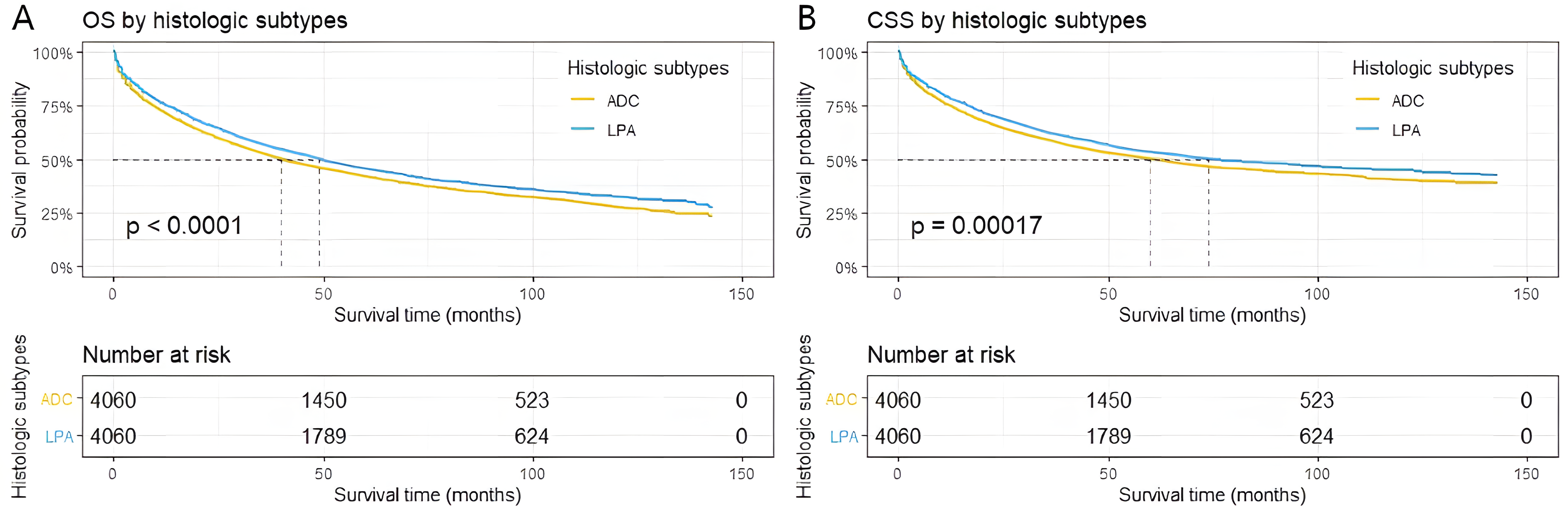
Compared with other rare histologic subtypes of lung cancer, such as papillary adenocarcinoma (11) and carcinosarcoma (12), our results suggested that the incidence of LPA was much higher. Our results also indicated that LPA patients were more common in older age and females, which is consistent with previous studies (13, 14). In addition, some clinicopathological features of LPA patients indicated a good prognosis, including smaller tumor size, fewer separate tumor nodules, less pleural invasion, and lower histological grade and stage. This is consistent with previous studies (15) and in line with the good prognosis of LPA (3, 13, 15). Moreover, LPA possessed some characteristics differing from other histologic subtypes of invasive pulmonary ADC, such as being more common in nonsmokers or light smokers, a preference for pulmonary peripheral location and being false-negative in positron-emission tomographic scans (13, 16). Clinically, asymptomatic at presentation or excessive airway secretion were more common in patients with LPA (17). In the genetic alteration profiles, EGFR mutations occurred in approximately 50% of patients with LPA, which was significantly higher than other subtypes (5), especially mutations in exon 21 (17, 18). However, KRAS mutations are much less common and account for approximately 10% of the LPA population (5). Compared with other histologic subtypes, a lower rate of ALK rearrangement and a higher rate of RET rearrangement were reported (6, 19, 20).
Most studies supported that patients with LPA had desirable survival outcomes compared with other subtypes of invasive pulmonary ADC. Surgery is still the superior option for LPA patients, whereas adjuvant chemotherapy, including oral fluoropyrimidines and platinum-based regimens, conferred no survival benefit on patients with LPA, regardless of the tumor stage (21, 22). In patients with advanced LPA, studies have suggested that taxane-based chemotherapy and pemetrexed might be effective and well tolerated (23, 24). With higher frequencies of EGFR mutations, EGFR-TKI therapy for advanced LPA demonstrated encouraging efficacy (9). Nevertheless, due to the lower expression level of programmed cell death-ligand 1, the efficacy of immune checkpoint inhibitors in patients with LPA may be poor (25-27). Moreover, multiple studies suggested that a higher percentage of lepidic growth patterns was associated with a lower risk of recurrence, and invasive component size was a better predictor for survival than overall tumor diameter (16, 17, 28, 29). Furthermore, no recurrence was observed in any of the 18 LPA patients with a maximum tumor diameter > 3 cm but the maximum diameter of the invasive area < 5 mm (30). Therefore, Suzuki et al. (30) proposed that LPA with an invasion of 5 mm or less can be regarded as minimally invasive ADC even if the tumor is larger than 3 cm in diameter. Unsurprisingly, our results suggested that primary tumor surgery was a major prognostic factor of LPA patients following histological grade and stage. In contrast, chemotherapy was far less important to the prognosis of LPA patients. Furthermore, our results suggested that radiotherapy had no significant effect on the survival outcomes of LPA patients. Regrettably, we could not explore the prognostic significance of chemotherapy regimens, targeted therapy, immunotherapy or the diameter of the invasive area.
In the current study, we identified that age, sex, marital status, primary tumor size, pleural invasion, histological grade, TNM stage, primary tumor surgery, and chemotherapy were independently associated with OS and CSS in patients with LPA. Notably, few patients with histological grade IV LPA were included in this study. Therefore, the nomograms we constructed to predict the survival outcomes were not suitable for patients with histological grade IV LPA. Similar to previous studies, our results suggested that treatment, tumor size and some demographic characteristics also had an impact on the prognosis of LPA patients, and we provided a statistical prediction tool that can incorporate and quantify the selected prognostic factors to estimate the survival outcome for an individual patient. Moreover, our nomograms were examined by C-index, ROC curves, calibration plots, and DCA curves, which demonstrated that the nomograms showed excellent agreement between the nomogram-predicted and actual survival outcomes of patients with LPA, as well as better prognostic capacity than TNM stage.
To date, this is the first time that the demographic and clinicopathological features, as well as the incidence of LPA, have been elucidated based on a large-scale population-based database. Meanwhile, this is the first nomogram predicting the survival outcomes of LPA patients, which could aid in personalized prognostic evaluation and clinical decision-making. However, there were still some limitations in our study, although the nomograms demonstrated good accuracy and applicability. First, nomograms were constructed based on retrospective data, and prospective external validation is needed. Second, some critical information, such as the diameter of the invasive area in LPA, tumor biomarkers, chemotherapy regimen, targeted therapy, molecular pathology, and genetic tests, was absent in the database. Moreover, the TNM staging information provided by the database is the result of the 6th edition staging system, instead of the latest edition staging system. Therefore, we could not analyze those variables or improve the prognostic nomograms in our study. Third, the patients were almost all Americans, and the results might be different in other races. Such drawbacks are inherent to almost all retrospective population-based studies. However, the large size and the long follow-up duration of the present study compensate to a great extent and provide comprehensive knowledge of LPA. Further prospective studies with more important information are needed for model improvement and independent validation.
{kind=link}
{kind=link}