Nephrolithiasis is a condition of having stones in the kidneys, which progressively lead to loss of renal function if untreated properly.1. The prevalence and incidence of kidney stones is increasing across the world.2. The prevalence report over single time period for United States revealed a steady rise between 1964 –1972 and then stabilization since the early 80’s. Germany, Spain and Italy also reported increase in prevalence in over single period report. Scotland however reported a decrease in prevalence from 1977 to 1987. Overall the prevalence of kidney stones in the 1980’s on average was 3.25% and 1990’s 5.64% with the highest prevalence reported on adult Uranium workers in Tennessee, USA (18.5%) and adults in North East Thailand (16.9). 2 The exact prevalence of the disease in Africa is not known, as it was found in the studies done in South Africa there are stone prone and stone free areas. Sudan and Ethiopia are some of the stone prone areas. Those countries have high prevalence of calcium oxalate stones about 70%.3 Though kidney stone disease is common in this country, there is no any documented study done about the prevalence of kidney stone disease in Eritrea. 4
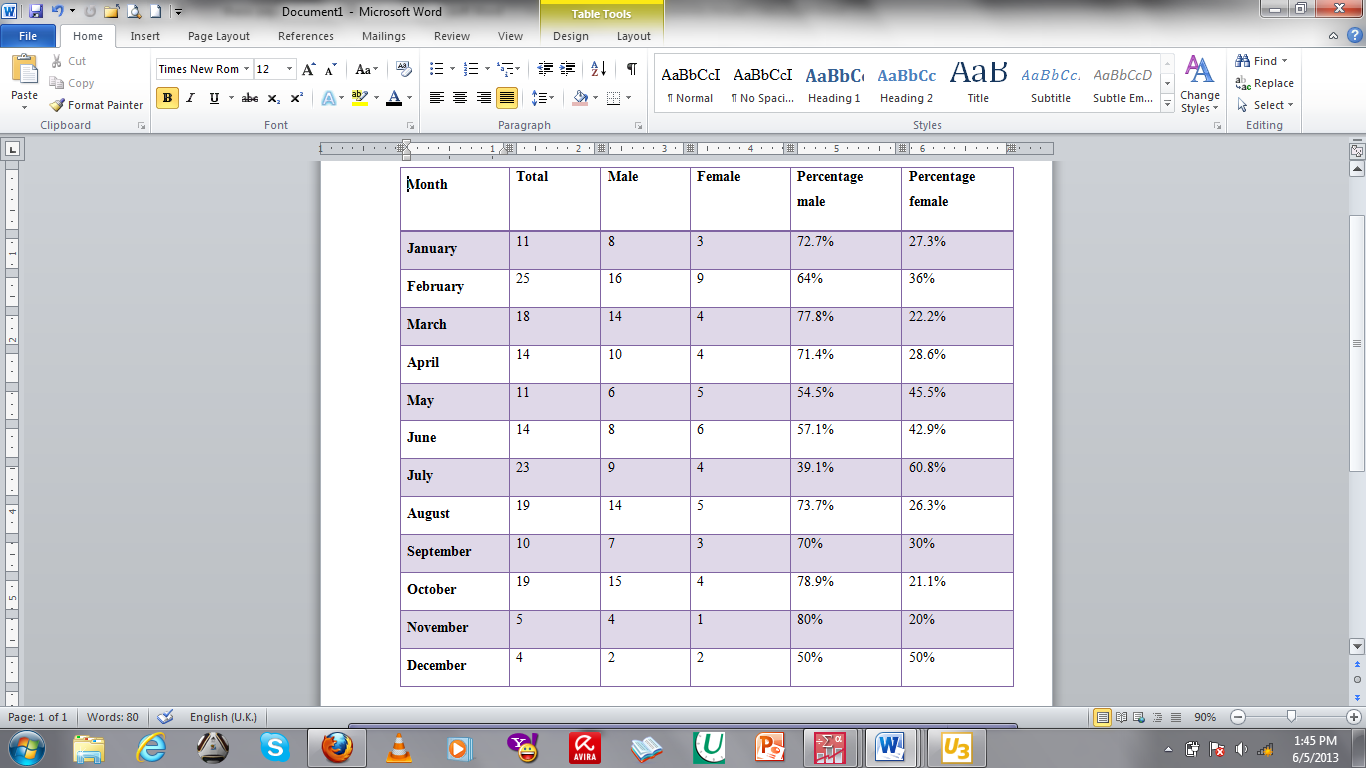
Men are more affected than women, Studies done in Japan and Iran showed that the ratio of kidney stone of men to women was 2.5:1 and 1.15:1 respectively. In Korea, prevalence rates decreased as men aged, but increased in women and peaked at age 60 to 69 years. Similar patterns were shown in Germany in the age group 14-24, in Milan 21-30, 60- to 79-year-olds in Korea, in the United States in the age group 20-29 and in Greece similar occurrence was reported in three different age groups (age < 20, age 30 to 39 years, and age 50 to 59 years).2 Studies done in Africa showed that Sudan and Ethiopia were prone to stone formation with higher prevalence in men than women.3
The prevalence of kidney stone generally increases as age increases. Studies done in Germany showed an increase in the prevalence as age increases, this trend was observed both in 1979 and 2001 reports. US kidney stone prevalence also increased with age. In 1978 prevalence in US men and women demonstrated a rise and fall pattern as the population ages, with peak prevalence occurring between age 60 and 69 years in men, and between age 50 and 59 in women. Studies done from 1976 to 1980 in the United States showed the prevalence to decrease in women over 59 and in Men over 69 but by the year 1991 the prevalence rate rose significantly as the age group increased. Milan, Italy, kidney stone an increasing prevalence was observed with increasing age among those living in Milan, but a prevalence decreased after age > 60 years. In 1998 Korean studies demonstrated a rise and fall pattern with Korean men prevalence increasing with age whereas in Korean women it showed an increase and decrease pattern peaking between 60 and 69 years.2.
In the United States, data relating Race and prevalence of kidney stone revealed kidney stone to be commonest among whites followed by Hispanics, blacks and Asians. However the prevalence has doubled for African Americans in the age group 60 to 74 comparing studies done in 1976 through 1980 and 1988 through 1994. For each race men have higher prevalence as compared to women in the same race.2. A study done in Benin, Nigeria showed the prevalence of kidney stone to be 6.3 per 100,000 of population. The ratio of male: female was 4: 1 with peak age being between the third and 6th decade of life. 13
Different factors have been associated with the increase in the prevalence of kidney stones. Environment, genetic, dietary changes and obesity have been known to contribute to these changes. Historical evidence shows that the first report of increase in kidney stone formation occurred during the 16th century when the demand for European stone cutters (Stein-Schneiders) increased, at which time the food production improved and corn became popular staple food. The consumption of foods rich in starch like corn contributed to obesity, risk factor to kidney stone formation.2.
Different dietary factors have been known to promote kidney stone formation. The intake of refined starchy foods and obesity has been linked to kidney stone formation. With the increase in the incidence of obesity studies also show that it correlates with the rise in the incidence and prevalence of kidney stone formation. Studies show that with the increase in the BodyMassIndex the prevalence of kidney stones and chronic kidney disease increased, however the prevalence ceased to increase after the BMI increased above 30. Obesity is associated with excess nutritional intake of lithogenic substances such as refined sugars, low fluid intake, calcium, oxalate, high sodium intake and purine-rich foods. Obesity is also associated with an increase in incidence of urinary tract infection. Patients with central adiposity or high waist-to-hip ratios appear to have the highest risk 11. A study conducted in the United States shows consumption of antioxidants to decrease the formation of kidney stones. Antioxidants alpha-carotene, beta-carotene, and beta-cryptoxanthin were significantly lower in those with kidney stones (-9.36%, -10.79%, and -8.48%, respectively than those without kidney stones6. kidney stone formation has also been linked to high dietary Zinc intake. A study showed increase in the prevalence of kidney stones in patients with high dietary zinc intake (>15 mg/day)7. It has been proposed that dietary calcium, potassium, and total fluid reduce the risk of kidney stone formation, while supplemental calcium, sodium, animal protein, vitamin C intake of >90mg/day and sucrose may increase the risk11. In younger female adults the intake dietary calcium was associated with decreased risk of developing kidney stone while supplemental calcium was not associated with any risk. However in older individuals the facts may change due to change in metabolism of calcium. In males < 60 years dietary calcium decreases the risk whereas in men >60 years dietary calcium does not seem to affect the risk. Intake of animal protein was associated with risk only in men with a body mass index < 25 kg/m2.11.
Different metabolic syndromes have shown to have impact on the formation of kidney stones. Diabetes is associated with an increase in the incidence of renal stones disease. The shared links between the metabolic disorder and kidney stone is insulin resistance. Furthermore, insulin resistance is thought to alter renal acid-base metabolism, resulting in a lower urine pH and increased risk of uric acid stone disease.2,5. A study showed that in patients with kidney stone disease the presence of hypophosphatemia, hypokalemia, hyperuricemia and hypercalcemia was 11%, 12.6%, 20%, and 5% respectively.8. The presence of Hypertension has shown to have impact on the prevalence of kidney disease.9.
Calcium oxalate stone formation was significantly associated with several coronary heart disease risk factors, including smoking habit, hypertension, hypercholesterolemia, and obesity11. In primary gout 39% of patients had urinary stones of which about 30% were silent and diagnosed only by ultrasonography11.other medical conditions associated with renal stone include hyperparathyroidism, hyperthyroidism, sarcoidosis, malabsorption (inflammatory bowel disease, ileal resection or bypass) and cystic fibrosis12 patients with injuries to the spinal cord are at high risk to develop kidney stone. Some of the reasons include catheterization leading to urinary tract infection along with urinary stasis and immobilization. Renal abnormalities which lead to urinary stasis such as polycystic kidney disease and other anatomical abnormalities increase the risk of kidney stone. Medullary sponge kidney, distal renal tubular acidosis and recurrent history of urinary tract infection also increase the risk of stone disease. 12
Different environmental factors have been linked to the increase in the prevalence of kidney stones. Warm climates and sunlight exposure have been linked to kidney stone disease. The possible theories include exposure to warm climate leads to dehydration, making the urine more acidic, a risk factor to stone formation.10. Sunlight stimulates the increased production of 25-hydroxycholecalciferol in the skin, which, after conversion to 1,25 dihydroxy-vitamin D by the kidneys, enhances intestinal absorption of calcium.
Elevated levels of circulating 1, 25 dihydroxyvitamin D have been found in patients with hypercalciuria and excess urine calcium is linked to stone formation, this occurrence was more common in men probably due to more sunlight exposure.10
Almost 85% of stones contain calcium with oxalate and phosphate either alone or combined. Calcium oxalate stones are made of monohydrate (COM) and dihydrate (COD) crystals. COM, the thermodynamically most stable form, is observed more frequently in clinical stones than COD, at a ratio of >2:1. The pathogenesis of calcium oxalate stone formation is a multi-step process and includes nucleation, crystal growth, crystal aggregation and crystal retention. Enucleation is the formation of solid crystals in urine; supersaturation plays a big role in this process. Naturally urine has inhibitors of crystallization, holding large amount of solute in the urine, however if solute reaches to a point where it cannot be held in urine then the process of enucleation starts. New crystals may form on pre-existing crystals called secondary enucleation. Epitaxy is a process whereby material of one crystal type is precipitated upon the surface of another whose lattice dimensions are almost identical, this process is important for the formation of calcium oxalate stones. The next important step is the crystal growth which starts approximately with enucleation. This process is determined by the molecular size and shape of the molecule, the physical properties of the
material, SS levels and pH. Crystal aggregation is the third process whereby crystals in solution stick together and form a larger particle. This process is determined by balance of forces, Tamm-Horsfall glycoprotein and other molecule may act as glue and increase viscous binding. Aggregate may further be stabilized by solid bridges formed by crystalline material connecting two particles. Normally tubular cells and crystal repulse each other hence inhibiting aggregation. In pathological conditions however, injury from free radicals results in sloughing of membranes from tubular membranes providing a condusive environment for enucleation and aggregation. Crystal retention is the next important process for kidney stone formation. A defective non-adherent property of the renal tubular epithelial cells promotes this process.14
Clinical pictures for patients with kidney stone may vary from acute pain to being asymptomatic. A study showed that in developing countries the prevalence of stones was underestimated after discovering kidney stones were diagnosed by renal sonography in 3% of non-symptomatic subjects.11. Manifestations include flank pain, urinary retention, renal colic, pyuria.13. Patients may present with moderate to severe colic, caused by the stone entering the ureter.
Stones in the proximal ureter cause pain in the flank or anterior upper abdomen. When the stone reaches the distal third of the ureter, pain is noted in the ipsilateral testicle or labia. A stone at the junction of the ureter and the bladder often causes dysuria, urgency,and frequency and may be mistaken for a lower urinary tract infection, hematuria is also common.15 Occasionally patients may present with ureteral obstruction which later results in hydronephrosis of the proximal kidney. Patients may also present with recurrent urinary tract infection. Colicky pain may radiate to the groin and as the stone descends down the ureter the pain may localize. The renal capsule and intestines share visceral innervations hence patient may also present with nausea and vomiting. Due to the severity of the pain it may mimic acute abdomen or pelvic condition but peritoneal involvement is absent.16
Helical CT without contrast is the preferred imaging study in patients with suspected nephrolithiasis. It has the advantage that it requires no radiocontrast material; it has the ability to show the distal ureters; it can detect radiolucent stones like uric acid stones, radio-opaque stones, and stones as small as 1to 2 mm; and it can detect complications such as hydronephrosis and intra-abdominal and renal disorders other than stones that could be causing the patient's symptoms. A study showed that CT scan done in 100 patients the sensitivity was 98% and specificity was 100%. Ultrasonography though convenient in that it does not expose to radiation has its own limitation. It is less sensitive in that it can detect stone in only kidney and proximal ureter. A retrospective study showed that ultrasonography when compared with helical CT scan had a sensitivity of 24% and a specificity of 90%. Ultrasonography may also miss stones smaller than 3 mm in diameter. Kidney- Ureter- Bladder x-ray has low sensitivity, misses out on radiolucent and small stones. Intravenous Urography although previously widely used has few advantages not to mention the risk of hypersensitivity to Iodine dye in patients.15
Several modalities of treatment are available for kidney stones. Urgent intervention is one option, indications include patient with obstruction, infected upper urinary tract, impending renal deterioration, persistent pain or vomiting, anuria, or high-grade obstruction of a solitary or transplanted kidney. Infection secondary to obstruction is manifested by fever, urinalysis reveling pyuria, bacteriuria, and leukocytosis, and the presence of urosepsis, in such cases intravenous antibiotics might be needed, intravenous ampicillin and aminoglycoside provide broad antibiotic coverage, although oral fluoroquinolones may be a reasonable alternative; the type of antibiotic may be adjusted once the culture results are known. During acute pain traditionally Narcotics where used, however Nonsteroidal anti-inflammatory drugs have been labeled as adequate analgesics. Non-steroidal anti-inflammatory drugs when acting on afferent arteriole provide adequate pain relief by reducing ureteral spasms and reducing diuresis. Other remedies for acute pain relief include acupuncture and resistive heating blanket set to 42°C. Because the pain is due to renal capsular distention, intractable pain is controlled by decompressing the obstruction. In rare instances, patients may have persistent vomiting; they patients also require decompression and intravenous hydration.16
Smaller stones tend to pass spontaneously. For a stone to pass spontaneously the size has to be 5mm or less. It has also been noted that as the stone size increases the likelihood of the stone to pass decreases. Two thirds of ureteral stones pass within four weeks. Here also as the stone size increases the mean time for passage decreases. It has been proposed that a ureteral stone which has not passed within one or two months of period is unlikely to pass at any given time. A stone which has stayed in the ureter longer than 4 weeks is associated with further complications such as renal deterioration, sepsis, and ureteral stricture. Therefore for the above mentioned facts it seems only reasonable to appoint patient for 4 weeks of observation. 16
Uric acid stones are the only stones that can be managed medically. At a urinary pH less than 5.5, uric acid is insoluble; solubility increases at a pH greater than 6.5. Alkalinizing the urine with potassium citrate (or sodium citrate or sodium bicarbonate) dissolves pure uric acid stones. A usual therapy practice is 20 mmol of potassium citrate orally two to three times daily, and later reassessment is needed to verify adequate urinary alkalinization (to pH 6.5 to 7). The time to dissolution varies with the size of the stone and the extent of urinary alkalinization. A 2-cm uric acid stone in urine with a constant pH of 7 takes approximately nine days to dissolve. Investigation can be repeated at one month to determine whether dissolution has occurred. Unless a stone is pure uric acid, oral dissolution therapy is not possible. If oral dissolution therapy fails, treatment should proceed as for a radiopaque stone.16
When managing renal stones the options of treatment depends on whether the stone is small or big. For stones less than 2cm the preferred option of treatment is Lithotripsy. It is most effective for stones in the renal pelvis with 76% of patients becoming stone-free and least effective for stones in the lower pole (59% stone-free). For this reason, for stones in the lower pole, only those smaller than 1 cm in diameter are treated with lithotripsy. The disadvantages of lithotripsy include perforation, bleeding, inflammation and disturbances in cardiac electrical signal transmission, leading to cardiac arrhythmias during treatment. It is contraindicated in pregnancy and coagulopathic states and is less effective in morbidly obese patients is contraindicated in pregnancy and coagulopathic states and is less effective in morbidly obese patients, lithotripsy is more likely to fail if the skin to- stone distance is more than 10 mm.17
For larger stones the preferred option of treatment is percutaneous nephrolithothomy. It involves inserting a needle through the skin into the collecting system and then dilating the tract. Instruments are then inserted through this tract to break up and remove stones. is indicated in patients who have renal or ureteral stones larger than 2 cm or lower-pole stones larger than 1 cm. Percutaneous nephrolithotomy is invasive and carries several risks as any major surgical procedure, some of the complications include sepsis, perirenal hematoma or bleeding, and injury to nearby organs, including pleurae, lungs, bowel, or spleen. 17
On treating ureteral stone, for the sake of selection of surgical options the ureter is anatomically divided into proximal and distal portions taking the iliac vessels as land marks for division. Shock wave lithotripsy is the preferred method for proximal stones; it is useful for stones less than 1cm. Different type of the machines has different intensities and produce fragments of different sizes and retreatment rates. Stones composed of calcium oxalate dihydrate or struvite fragment more effectively than stones made of calcium oxalate monohydrate, Calcium phosphate, or cystine. Proximal ureteral stones that are larger that1 cm are treated more effectively by ureteroscopy than shock-wave lithotripsy. In a retrospective analysis of ureteral stones treated by ureteroscopy or shock-wave lithotripsy, the stone-free rates for stones of 1 cm or greater were 93 percent and 50 percent, respectively. For stones less than 1 cm, the stone free rates between the two groups did not differ significantly (100 percent and 80 percent, respectively).16
For distal ureteral calculi, the preferred treatment is controversial. In a prospective study patients with distal ureteral stones (mean size, 7 mm), shock-wave lithotripsy and ureteroscopy had similar results in stone-free rates. The percentage of patients who were in favor of repeating the procedure was slightly greater for shock-wave lithotripsy (100 %) than ureteroscopy (87 %).
Although there are no evidences to support the theory applying shock wave treatment to the distal third of the ureter to women with child bearing age might affect the ureters. Ureteroscopy may be used in women of childbearing age if not pregnant. Regardless of the mode of treatment used, the composition of all stones should be determined. Ureteroscopy with use of special laser is effective for stones of all compositions and sizes. This technique involves passing the ureteroscope retrogradely through the urethra, bladder, and ureter to the stone under video guidance. The laser is delivered through a small-diameter fiber passed through the ureteroscope. The fiber tip touches the stone, the laser is discharged, and the stone absorbs the laser’s energy, producing photo thermal lithotripsy. In a series of 504 patients treated with the use of this approach, stones were eliminated in 98 percent of those with distal ureteral calculi, 100 percent of those with middle ureteral calculi, and 97 percent of those with proximal ureteral calculi. Ureteroscopy is less expensive than shock-wave lithotripsy, but it is more time consuming and technically more demanding. 16
To prevent recurrence of kidney stones several measures could be taken. To prevent calcium oxalate stones one must treat the underlying causes of calcium in the urine. Calcium oxalate overgrowth on plaque is directly linked to calcium oxalate supersaturation, which is strongly linked to high urinary calcium excretion. Hypercalciuria can be caused by primary hyperparathyroidism, sarcoidosis, vitamin D excess, corticosteroid treatment, renal tubular acidosis, hyperthyroidism, and malignant neoplasms, it can also be idiopathic. In the latter hypercalciuria can be prevented by restricting sodium intake and giving thiazides. Thiazide diuretics lower urinary calcium excretion and promote mineral retention. Restriction dietary calcium however is not recommended as it may promote unbound oxalate in the urine, a precursor to calcium oxalate stone.
Distal renal tubular acidosis is defined by systemic metabolic acidosis, alkaline urine, hypokalemia, hypercalciuria, hypocitraturia, and nephrolithiasis. The chronic metabolic acidosis results in loss of bone calcium, contributes to hypercalciuria, and is responsible for the hypocitraturia. Stone formation is the result of excessive urinary calcium excretion and persistently alkaline urine. Treatment with sodium bicarbonate or potassium citrate corrects the metabolic acidosis, reduces the loss of calcium from bone, corrects hypokalemia, and increases urinary citrate.
Elevated urinary uric acid excretion (> 800 mg/day in men, > 750 mg/day in women) is associated with formation of calcium stones. Treatment includes lowering uric acid stones with Allopurinol. Hyperoxaluria may be the result of high dietary intake, increased gut absorption, malabsorption of fat or simply genetic. Correction of hyperoxaluria includes dietary correction and appropriate management of underlying conditions which lead to fat malabsorption. Struvite stones are the result of chronic upper urinary infection with urease-producing bacteria like proteus spp Treatment includes eradicating bacteria and removing the stones which harbor the bacteria.
Cystine stone disease is seen in people who have inherited an autosomally recessive gastrointestinal and renal tubular transport disorder of four amino acids, i.e., cystine, ornithine, arginine, and lysine. Of these four amino acids cystine is the most insoluble and precipitates in urine. To prevent cystine stone disease treatment should include hydration adequately to achieve daily urine volumes of 3 to 3.5 L, alkalinization of the urine to a pH higher than 6.5 with potassium alkali or sodium bicarbonate reduction of protein and sodium intake to decrease cystine excretion. If these measures fail, D-penicillamine, tiopronin, or captopril can be given to convert the cystine to a more soluble disulfide cystine drug complex. 15
{kind=link}