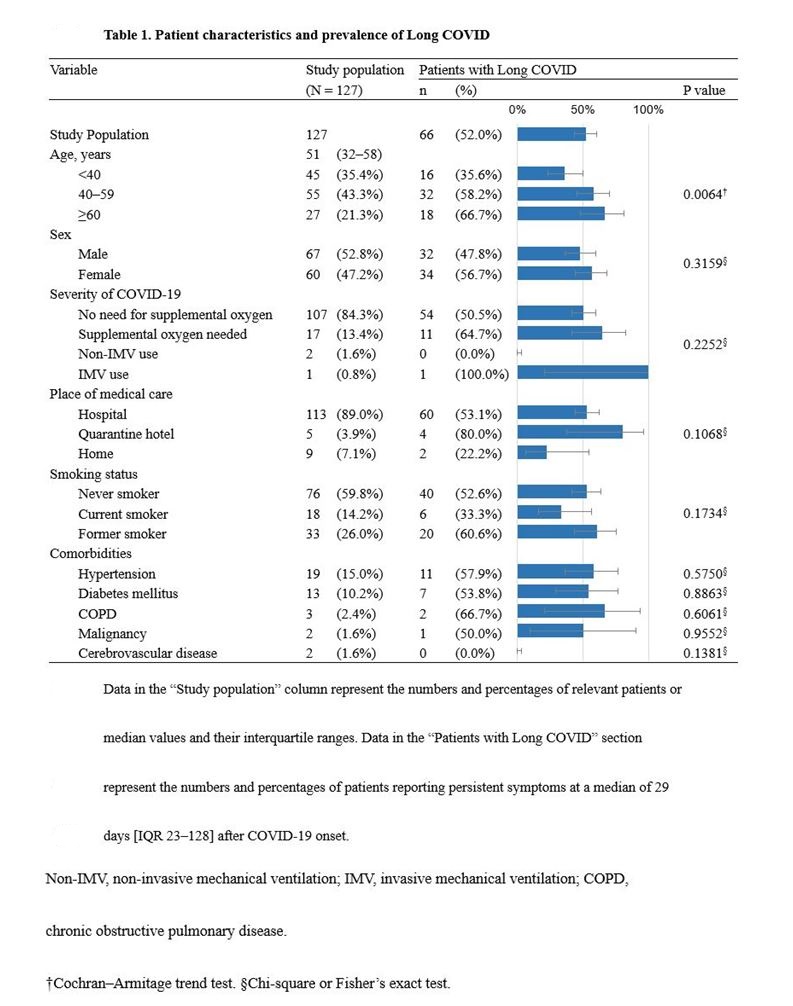
To investigate the clinical characteristics of Long COVID, we conducted a cross sectional self-administered questionnaire survey in patients treated at two major COVID-19 hospitals in Hiroshima Prefecture, Japan. Analysis of the responses from 127 recovered patients showed that 52.0% had sequelae at a median of 29 days [IQR 23–128] from COVID-19 onset. The prevalence rates of post-acute or prolonged sequelae of COVID-19 reported in the literature vary considerably depending on the geographic location of the study area and patient background factors [6]. In a recent Japanese follow-up study of 63 patients who recovered after hospital-based treatment, sequelae were reported in 76% at 14 days, in 48% at 2 months, and in 27% at 4 months after COVID-19 onset [12].
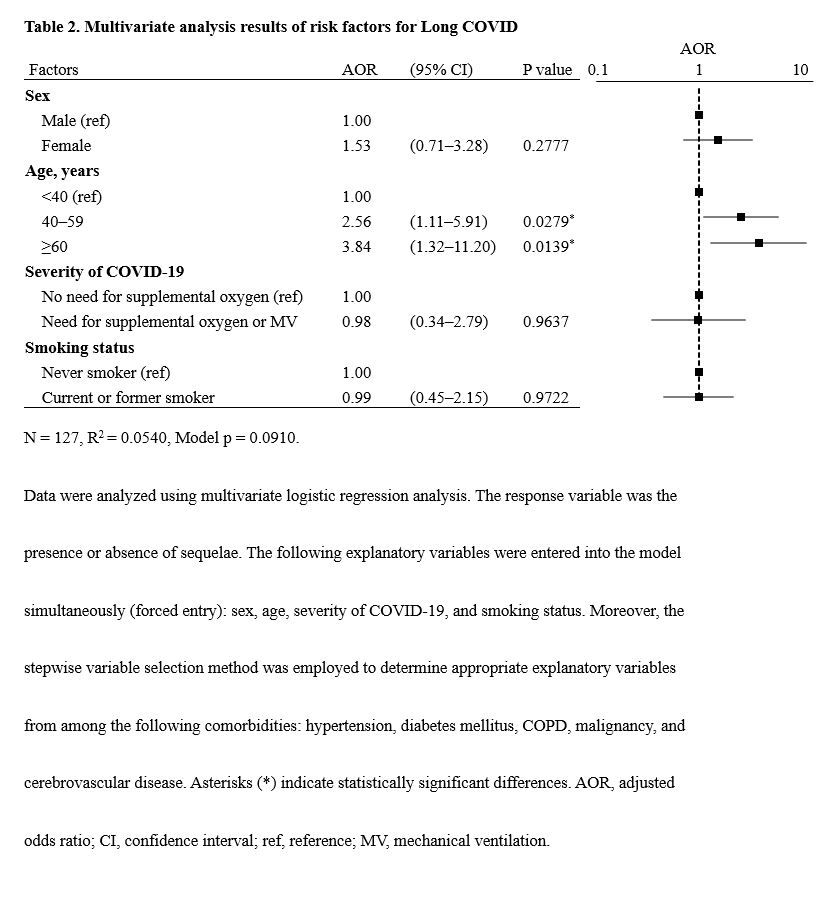
In our study, multivariate logistic regression analysis revealed that older age was an independent and significant risk factor for sequelae. Our findings are consistent with previous research showing that Long COVID was more likely with increasing age [13], emphasizing the need for follow-up focusing on Long COVID in elderly patients.
Long COVID symptoms are wide ranging, and include olfactory disorders, taste disorders, cough, fatigue, and dyspnea. COVID-19 affects various tissues and organs, such as those in the respiratory, cardiovascular, and neurological systems. Possible mechanisms underlying Long COVID may include immunologic aberrations and inflammatory damage in response to the acute infection, as well as virus-specific pathophysiologic changes [14]. ACE2, the major cell entry receptor for SARS-CoV-2, is extensively expressed in numerous human tissues and organs. Respiratory and other sequelae of Long COVID have been found to be common in organs with high ACE2 expression [15, 16]. In our study, patients aged ≥60 years were more likely than other age groups to report fatigue, palpitations, dry eye or mouth, dyspnea, and sputum production, whereas patients aged <40 years reported lower prevalence rates of all sequelae except for olfactory and taste disorders. Indeed, the fact that olfactory and taste disorders were more common in younger patients was consistent with a previous report [17], and may help distinguish symptoms that are more likely to persist in specific age groups.
Even in patients with mild COVID-19 who did not require supplemental oxygen or ventilatory support, sequelae were reported by 50.5% of them. Previous studies also reported that 53–55% of non-hospitalized COVID-19 patients had Long COVID symptoms [17, 18]. These findings suggests that COVID-19 patients should be followed up for persistent symptoms regardless of severity of COVID-19.
Regarding the impact on occupational performance, 17.4% of the post–COVID-19 patients had moderate or severe impairments (WFun scores ≥ 21). In a previous study that used the WFun questionnaire to investigate degrees of impairment in work performance associated with insomnia, 20% of control subjects without insomnia and 34% of subjects undergoing insomnia treatment had WFun total scores ≥21 [19]. This simple comparison suggests that post–COVID-19 conditions may influence work performance to only a limited extent.
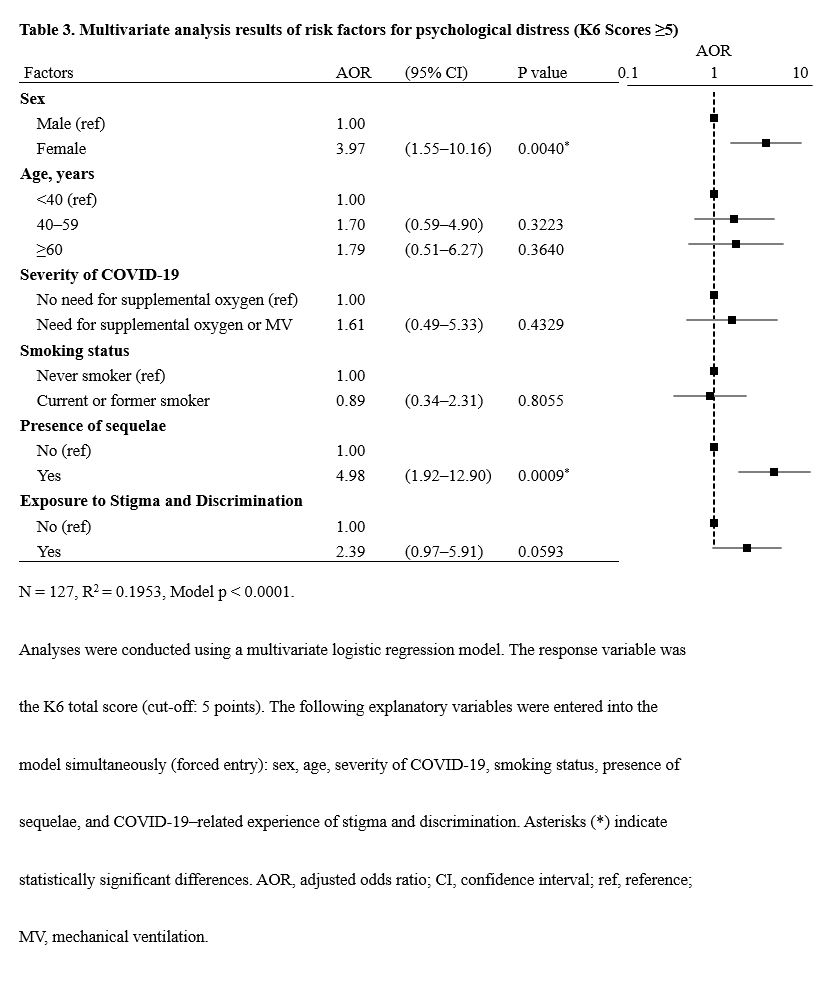
The prevalence of possible mood or anxiety disorders (K6 total scores ≥ 5) were 17.9% for males and 45.0% for females. Compare to the result of the general population (males 24.8%, females 29.6%) [20], the prevalence was lower in male patients and higher in female patients. The results of logistic regression analysis revealed that female sex and the development of sequelae after COVID-19 were independent and significant risk factors for post–COVID-19 mood or anxiety disorders. For female patients as well as patients with sequelae should receive long-term follow-up with a particular focus on the risks of mood or anxiety disorders.
Overall, 43.3% of our study participants reported exposure to stigma and discrimination related to COVID-19, suggesting that patients may face social challenges as they resume their everyday activities after recovery. Further expansion of the support system for ex-COVID-19 patients by the government and medical institutions and measures to eradicate discrimination are needed.
{kind=link}
{kind=link}
{kind=link}