The contemporary treatment for LARC provides long-term survival in most patients, but acute and late sequelae are major setbacks and jeopardize the successfulness of medical interventions. Investigation on new treatment strategies should maintain efforts to improve disease control rates, but optimization of the quality of life after successful treatment becomes a prime directive. In consonance, our randomized study was designed to compare clinical response between capecitabine and 5-Fu/Lv combined to radiotherapy in neoadjuvant setting, but also included a dedicated QOL analysis. In the present study we assumed that EORTC’s QOL scores would reflect clinical differences in disease responses according to treatment group results. After neoadjuvant treatment, despite no difference in QLQ-C30 scores between patients receiving capecitabine or 5-Fu/Lv was found, patients in group 1 (capecitabine) reported less miccional problems (15.3 pts mean difference), less gastrointestinal problems (-15.3 pts mean difference), less defecation problems (11.8 pts mean difference) and more sexual satisfaction (13.3 pts mean difference) in CR38 questionnaire specific colorectal modules. Coincidently, the clinical response rate (70.0% vs 53.3%) and the pathological complete response rate (23.3.% vs 10.0%) were higher in the capecitabine group, although not statistically which might have been explained by the sample size enrolled in the study. No previous publications compared QOL after these two drug regimens in neoadjuvant setting, but some reports compared these two drugs in adjuvant or palliative settings. A nonrandomized Taiwanese study published in 2015 evaluated 123 elderly stage III patients after adjuvant CT compared QOL and treatment costs of capecitabine vs 5-Fu/Lv, associated or not to oxaliplatin(34). After adjusting confounding variables and baseline characteristics, QOL using capecitabine was not inferior to 5-Fu/Lv and reduced costs. In accordance, two previous studies compared palliative treatment in metastatic colorectal cancer using capecitabine and 5-Fu/Lv in combination to oxaliplatin showed no difference in QOL between treatment groups(35, 36). Nevertheless, comparing the moments before and after neoCRT we balanced the effect of surgical resection and excluded the interference of oxaliplatin, which allowed a direct comparison of the two drugs in combination to radiotherapy.
The second question to be answered was regarding the functional results after sphincter preservation, which was an important endpoint in our study. Combining accurate preoperative imaging (MRI and EUS) to modern surgical techniques, the sphincter preservation rate was 81.6% in our study, considering all patients. We have accomplished to reestablish the intestinal continuity using coloanal anastomosis and/or intersphincteric resection after good clinical responders even with low rectal cancers close to sphincter complex, although our functional results were often suboptimal (mean Wexner score of 9.2). Interestingly, no functional difference was observed after ISR compared to LAR.
Both neoadjuvant schemes were effective in ameliorating general cancer symptoms and health status after neoCRT(T1) compared to baseline (T0), expressed as improvements in role functioning, global health status and C30SumScore scales of QLQ C30 and reduction in defecation problems of CR38 questionnaire, and no worsening of any domain of both questionnaires. In contrast, the adverse effects of rectal resection in QOL were evident: four of the C30 scales and three of the CR38 scales had worse scores comparing T1 to T2. Not surprisingly, patients had nonsignificant improvement in QOL six months after rectal resection, except for weight loss and sexual functioning despite receiving many cycles of adjuvant chemotherapy from T2 to T3. This time interval may have allowed improvement in patients perception of surgical morbidity. And although our sphincter preservation rate was over 80%, patients had to deal with temporary stomas for at least six months.
Finally, we included a late fecal continence evaluation one year after stoma reversal using the Wexner score, which has been recently translated and validated in Portuguese(33). We found an average high score of fecal incontinence that did not correlate to anastomosis level but correlated to QOL scores of diarrhea and defecation problems.
Our participants have never recovered from some sequelae of the treatment even at late evaluation after a median time interval of 49 months. Comparing to basal evaluation(T0), patients improved from general cancer symptoms (Global Health Status), ameliorated on weight loss and constipation, but developed male sexual disfunction. Comparing the late evaluation (T4) to the postoperative period (T2), patients had improvement in role functioning, weight loss, miccional problems and sexual functioning, which may reflect that some autonomic sequalae can ameliorate with time, but also can reflect a tendency of patients to change the perception of the same condition over time, for example if their cancer is controlled, a phenomenon called “response shift”(37, 38). The literature supports the findings of symptom improvement over time. A study from the Netherlands identified worse C30SumScore, physical functioning, fatigue and dyspnea in patients who received adjuvant chemotherapy compared to observation, but this difference disappeared 12 months after surgery(39). Other studies demonstrate stabilization of LARS one year after surgery(40) and that patients after long time follow-up still present significant disfunction (41).
Concerning the specific colorectal cancer module, the CR38 was commonly used in adjunct to QLQ-C30 to measure specific domains of quality of life in colorectal cancer patients, but criticism has emerged because questions concerning sexuality are often unanswered on CR38; these questions were suppressed or revised in the CR29 version(22). CR29 emerged later and was in validation when we started our study. Indeed, in our study few patients answered questions about sexual problems (only were 4 available to compare T0 and T1) and sexual satisfaction (only 19 of 61 were available).
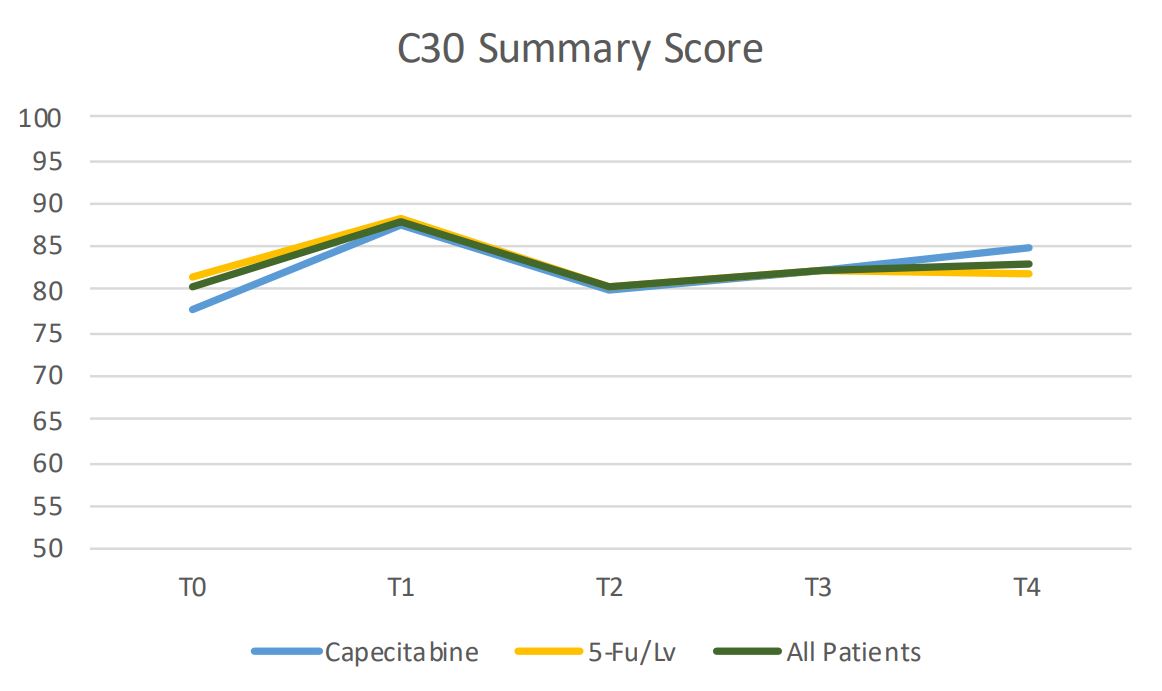
Our study was the first to use the C30SumScore to compare results of QOL over time in five moments beginning at pretreatment levels, and it detected significant differences in QOL after neoCRT and rectal resection. After neoCRT patients reported an increase in 6.1 points in C30SumScore and after rectal resection a decrease in 7.8 points in mean scores. The C30SumScore appears to add relevant information to clinical practice allowing comparison between treatment groups and detecting relevant temporal changes in QOL.
Unfortunately, our study leaves unanswered an old dilemma concerning better selection of patients for sphincter preservation after low rectal cancer resection. We did not detect differences in Wexner scores comparing patients with LAR to ISR, and both groups showed moderate to high levels of incontinence (mean 9.1 versus 10.0 points, respectively). A meta-analysis published in 2015 including 13 studies from 2001 to 2015 comprised data from 1805 patients using QLQ-C30 and CR38(23). Their main objective was to compare QOL in patients submitted to LAR vs APR, and QOL questionnaires were applied after 12 months of surgery. Patients with sphincter preservation had better social functioning, better body image but more symptoms of constipation. One study from Spain evaluated QOL compared APR versus LAR in 84 patients after neoCRT and Surgery (42). After a mean follow up of 48.7 months, no difference in QLQ-C30 scores was detected. Using the CR29 questionnaire, only stool frequency score was increased in LAR patients (33.3 vs 14.3 points). Another study compared QOL and functional results using Wexner score in 14 patients submitted to ISR versus 22 patients submitted to APR and perineal colostomy(43). ISR patients had worse Physical Functioning (84.1 vs 100.0 points) but less Defecation Problems compared to perineal colostomy (57.1 vs 90.5 points). Wexner score was similar between two groups (median 11 in ISF versus 10 in APR), which was comparable to our results of ISR (median Wexner score of 10). A matched group analysis from Heidelberg, Germany, compared QOL results of LAR, ISR and APR in 131 patients from a prospective database (44). They found that physical functioning scores were better after LAR and ISR compared to APR (82.2 and 80.2 vs 69.9 points), but constipation and diarrhea were both more frequent in LAR and ISR compared to APR. ISR had mean higher Wexner score compared to LAR (12.9 vs 9.5), a difference that was not significant in our series. A previous study from Illinois, USA, also found better physical functioning scores after sphincter preservation in a retrospective study (94 vs 87 points) but also more constipation (16 vs 8 points) and decreased sexual functioning (27 vs 76 points)(44). These suboptimal functional results after curative resection of low rectal cancer motivates investigation of less aggressive approaches to good clinical responders, including the nonoperative management that has been explored in recent literature, including our own institution’s experience(45, 46).
New strategies are under investigation to decrease toxicity and QOL impairment. Avoiding radiotherapy would probably reduce a degree of pelvic toxicity ameliorating anorectal function after rectal resection, and some studies demonstrated promising response rates using isolated neoadjuvant chemotherapy(47, 48). One tendency in investigation by our group is the total neoadjuvant treatment, in which all cycles of systemic chemotherapy are delivered before rectal resection with the addition of short-course radiotherapy (SHORT-ICAR Trial, ClinicalTrials.gov Identifier: NCT04674696). This strategy is aimed to improve response, increase compliance rates, prevent distant relapse, allows stoma reversal one month after TME, and the possibility of organ preservation after clinical complete response.
Finally, our study was limited due to incomplete accrual which may have limited the statistical power to detect small outcome differences between the two treatment arms, as only 63 of 96 patients were randomized after two years because some stage I and many Stage IV patients were later excluded after ultimate radiological review. Nevertheless, we were able to show significant difference in QOL in different phases of treatment combining the two treatment arms. We also did not include manometric evaluation, which would give additional information regarding the suitable candidates to sphincter preservation in low rectal cancer cases. Despite this possible caveat, manometry is not widely available as it depends on dedicated equipment and expertise, and many QOL of studies after rectal cancer treatment do not report manometry data. Most studies, including ours, focus on patient reported outcomes, as the Wexner scale and EORTC questionnaires, which make our results comparable to literature and applicable into clinical practice.
{kind=link}