Overall Effect of Family Intervention
This study aimed to quantitatively examine the effect of family interventions on the PA and SB in children aged 2.5–12 years by synthesizing the available literature in this field of inquiry. Through the combined 11 studies included, we found that family intervention could effectively improve the PA of children aged 2.5–12 years, especially for daily steps, but there was no obvious effect on SB.
Comparison with the Findings from Previous Reviews
Findings of this study indicated that family interventions have a positive effect on PA in children aged 2.5–12 years and our study is therefore a valuable extension of two published systematic reviews and meta-analysis [48, 49]. A meta-analysis provides evidence that school-based interventions can be effective in increasing PA enjoyment in children [48]. Jane’s [49] meta-analysis, based on school and family interventions, found that family interventions (involving children and parents) had better PA improvement than school interventions (only children). On this basis, when our study concentrate on family interventions, it still found that a significant intervention effect on PA in children. This study may provide additional information and be valuable contribution to this area of inquiry from family intervention and PA.
Indeed, a growing body of evidence has shown the benefits of intervention on children’s PA [47, 48], however, which index of PA is more sensitive to family intervention remains unclear. Among children previous reviews suggested that neither active play interventions [50] nor school-based interventions [51] have an effect on moderate-to-vigorous PA (MVPA). In accord with previous studies, findings from our study align with the previous points indicating that family interventions have no effects on MVPA. However, we found that family interventions significantly improved the children's daily step of 1,006 steps per day. Among previous reviews suggested that positive relationships between daily steps and physical fitness were observed [52]. Daily steps is an excellent indicator of health-related outcomes [53, 54]. Some studies suggested converting MVPA to steps because daily steps were easier to recognize generally[55]. The reason why our findings have no significant improvement on MVPA but improve daily steps may be the increased activity comes from LPA, not MVPA. Although PA guideline recommended to engage in sufficient MVPA to obtain health benefits from PA [56], previous reviews revealed that engaging in more LPA is also good for children's health [57, 58]. Therefore, we cannot ignore the potential health effects from family interventions to enhance LPA.
Nevertheless, the results of our review showed that family intervention had no significant effect on SB in children aged 2.5–12 years. It is a disappointing outcome for public health practitioners and researchers who consider the family a promising setting for interventions [17]. Previous school-based [51] or classroom-based [59] interventions have also been ineffective for SB. In general, family interventions design may focus more on PA logically not SB. Future research should consider the differences and concerns between PA and SB in study design.
Analysis of Influencing Factors
The result of subgroup analysis expressed that family interventions were more effective in increasing PA levels in certain subgroups, for example, intervention focus “PA only”, “low risk of bias”. In addition, our review showed that age may be one of the factors influencing the effectiveness of family interventions. How do these findings compare to those of other published studies? A number of studies focused on preschool children found no changes in PA and SB following PA interventions [60, 61]. However in this study, family intervention had a significant effect on PA in children aged 6–12 years. With the growth and cognitive development, the cognitive ability of school-age children (6–12 years old) was better than that of preschool children [62], and they also had a better understanding of family intervention and PA. At this time, parents could set a good example, or they live in a PA positive family, which can had a profound effect on a child's PA. Therefore, well-designed and targeted RCTs were needed for children of other ages in the future.
The study also demonstrated that intervention duration affect the effectiveness of family interventions. Intervention duration were categorized as “> 10 weeks” and “≤ 10 weeks” based on characteristics of included studies. It was found that interventions less than 10 weeks may have a more significant impact on PA improvement. The short-term (≤ 10 weeks) intervention effects may be attributed to the curiosity of the participants in the early stages of the intervention, and they are willing to participate in the implementation [63]. Over time, the decline in the interest and compliance of the participants led to the intervention effect not being maintained.
Strength and Limitations
This study has demonstrated several strengths. First, to the best of our knowledge, this is the first meta-analysis to quantitatively examine the effect of family interventions on PA in children aged 2.5–12 years, which provides additional insight in the field of family interventions and PA. Second, the meta-analysis is based on data from controlled trials studies regarded as a study design that substantially reduces selection bias and has a good comparability.
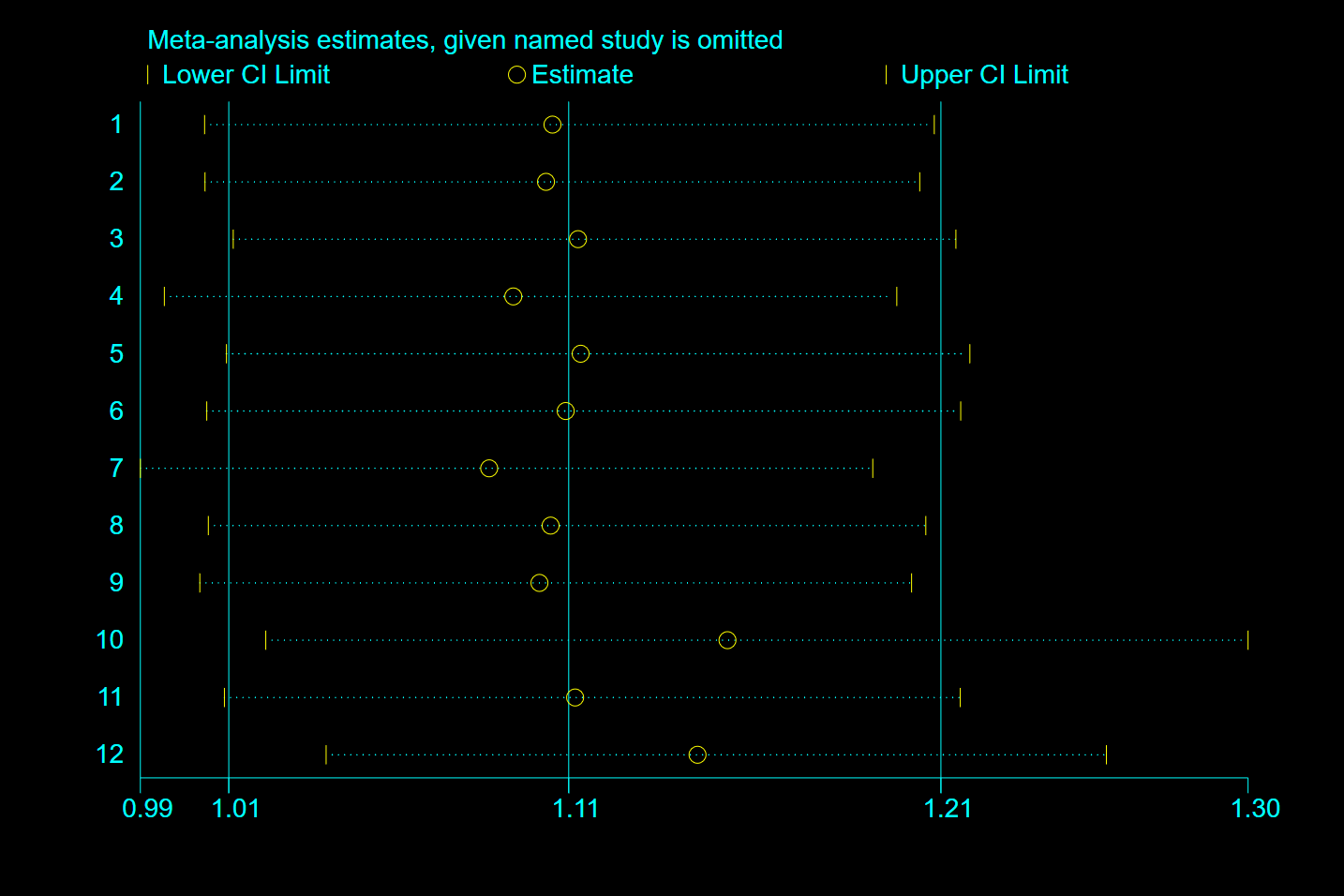
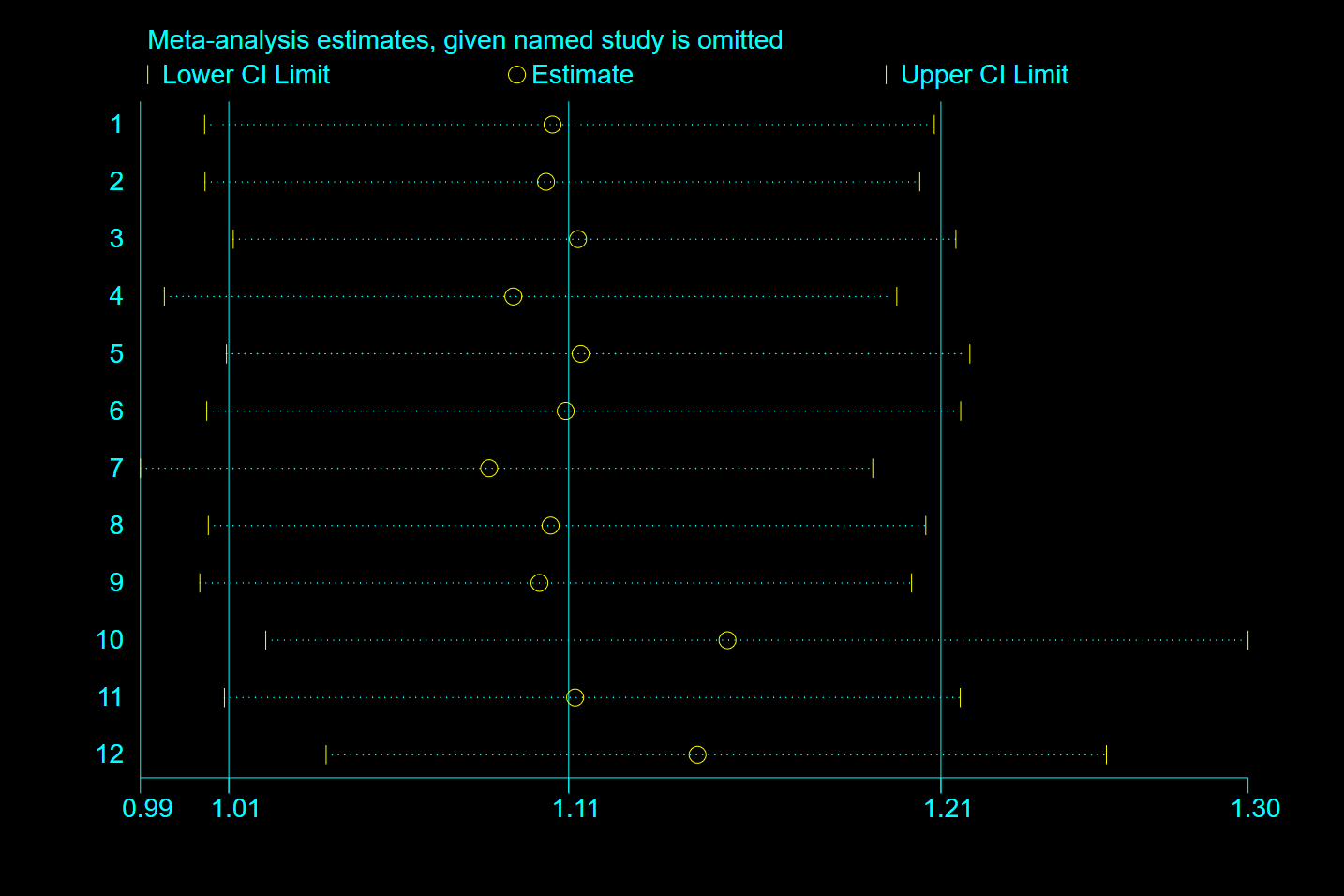
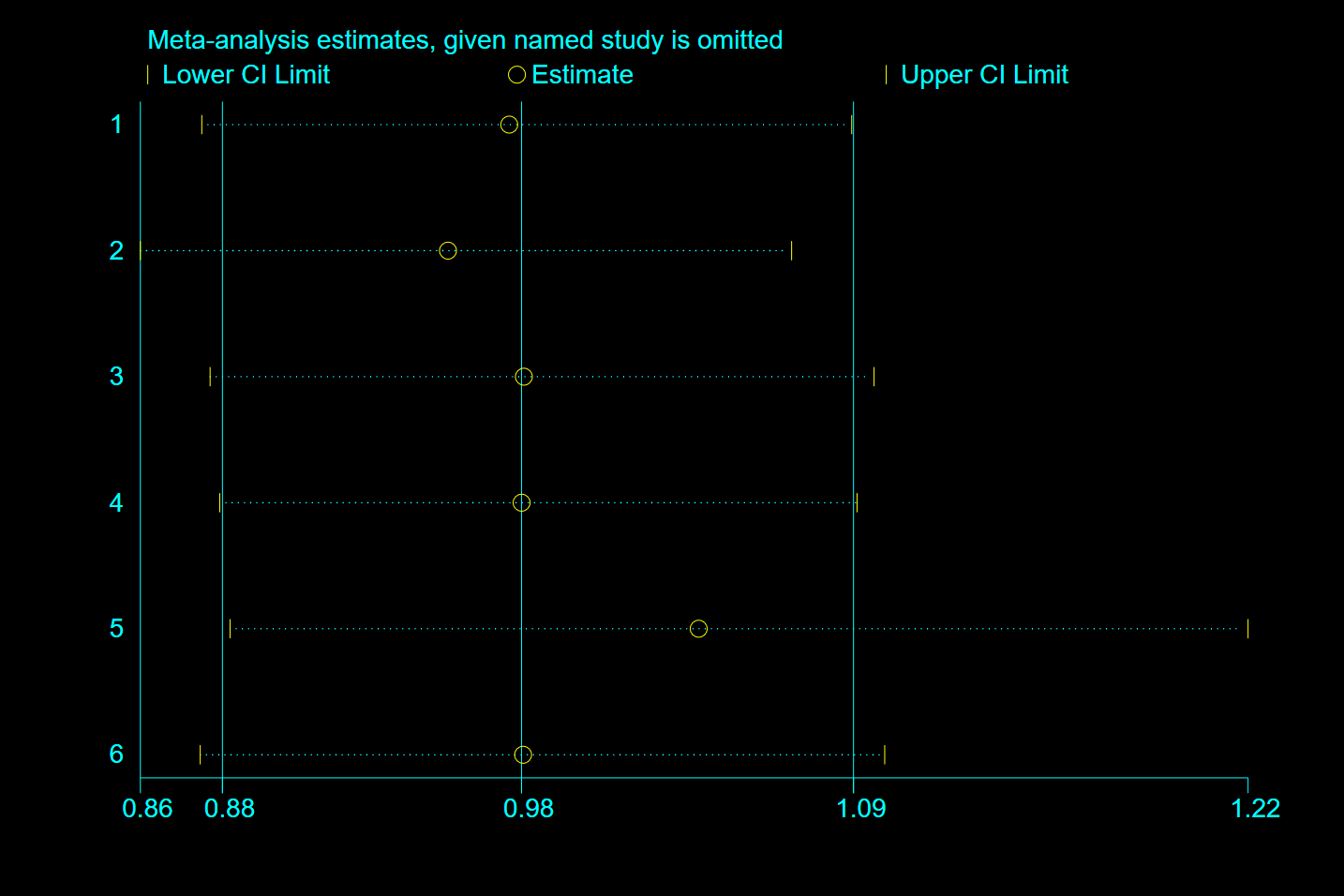
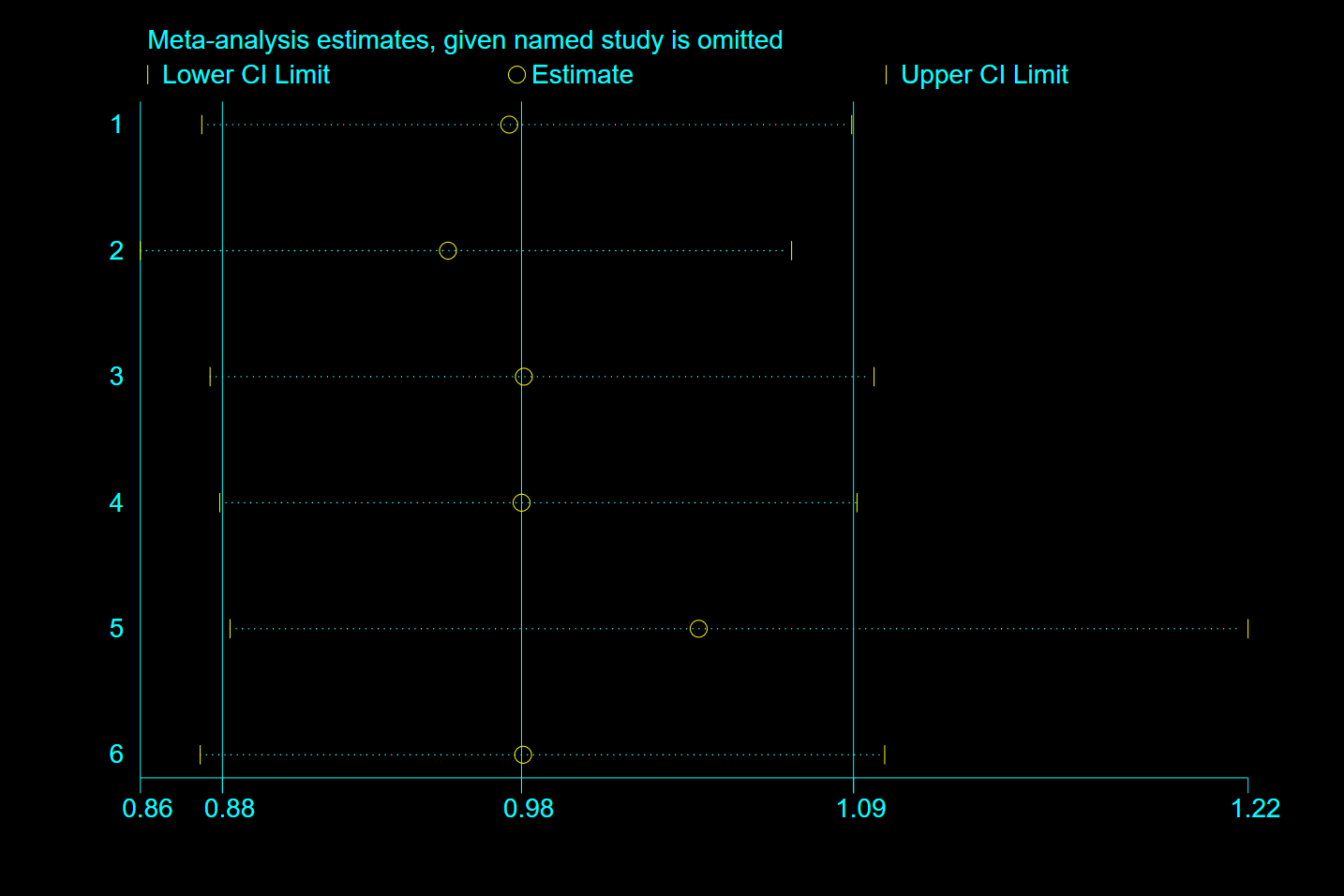
There were also some limitations in this study. First, most of the included studies was distributed in developed countries, so the research results were not widely representative. However, this study has included as much as possible the latest and most comprehensive research related to this proposition. Second, the family intervention programs (focus, means, duration) varied across included studies, which may lead to estimation bias of the overall effect. However, sensitivity analysis showed that the reduction of any one of the included studies did not significantly affect the combined results of this study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}