Our previous study established a grading system for limbal dermoids for clinical diagnosis and revealed that a lower grade dermoid was associated with better vision postoperatively [16]; however, little research has been conducted on visual function evaluation and vision reconstruction postoperatively. In this study, the LD patients exhibited obvious visual impairment in visual acuity and contrast sensitivity compared with the normal children, as many factors can influence the ability to discern contrast, such as the media opacities caused by the remaining focus, the stray light and glare sources induced by astigmatism and background illumination [4, 5]. Most epibulbar dermoids were excised with lamellar excision, and the remainder were excised with lamellar keratoplasty or eccentric sclerocorneoplasty. Hussein et al. [17] identified astigmatism greater than 1.5 D preoperatively and postoperatively as a risk factor for amblyopia. The mean spherical and astigmatic refractive errors in our participants were -3.78±3.71 D and -4.92±2.91 D, respectively, which were deemed to be associated with a high risk of amblyopia, while no conclusions were drawn regarding whether surgical resection facilitated amblyopia treatment or improved visual outcome. Our study indicated that obvious CSF impairment was observed in these LD children. In Nielsen and Hjortdal’s [4] study, the patients underwent posterior lamellar keratoplasty and had similar VAs and refractive statuses. The mean log CS was 1.06±0.25, compared with 0.49±0.15 in our study, in which Nielsen’s patients showed better CSF performance. We deduced that this is because the lamellar keratoplasty procedure could help to rebuild visual function, including CSF [4, 18].
These patients showed worse visual function than the children who had the same visual condition under the optical defocus. Optical defocus was used in this study to simulate the visual conditions of LD patients, which did not degrade binocular function and was the most permissive for binocular function [15]. The LD children exhibited obvious contrast sensitivity function impairment, especially at high spatial frequencies, compared with the corresponding optical defocus group, at almost each spatial frequency ranging from 1 to 0.04 LogMAR BCVA. Although refractive errors have been corrected prior to visual function evaluation, visual recovery may be dependent on further changes in the subepithelial and host stroma, ultimately leading to light scatter and amblyopia [19]. Management of amblyopia must continue after surgical excision to yield optimal results when or if the surgery is done at a younger age.
The term “perceptual learning” describes a process whereby practicing certain visual tasks leads to an improvement in visual performance [20]. Visual performance can be improved with repetitive practice of specific controlled visual tasks. These repetitive tasks initiate neural modifications that can lead to improvement in neuronal efficiency [21]. It should be emphasized that the patients had not shown any improvement with patching for 6 months. Nevertheless, they improved remarkably by training using the perceptual learning technique. The mean BCVA increased from 0.67±0.09 to 0.32±0.09, with an improvement of 0.35, under perceptual learning, and the AULCSF in the contrast sensitivity increased from 0.49±0.15 to 1.06±0.20, which is encouraging and reveals a positive trend. Polat et al. [11] studied 54 adult amblyopic patients who were randomized to a perceptual vision treatment program or a placebo vision training program for amblyopia. Pretreatment visual acuity in both study groups was 0.42 logMAR, and this improved by 2.5 lines in the perceptual vision treatment group, with no improvement in the control group [22]. It is likely that the advantage of perceptual learning is due to an active task that the subject is required to perform, whereas patching is passive [23]. More importantly, perceptual learning involves specifically training spatial frequencies within a range that can be improved. It is worth noting that the improvement of CS only appeared at the low and middle spatial frequencies, not at the high spatial frequencies. However, the middle and high spatial frequencies have been documented to be particularly useful for target detection and identification tasks, even in patients in whom visual acuity is not excellent [24]. We deduced that the high spatial frequencies require better visual acuity to recover [25].
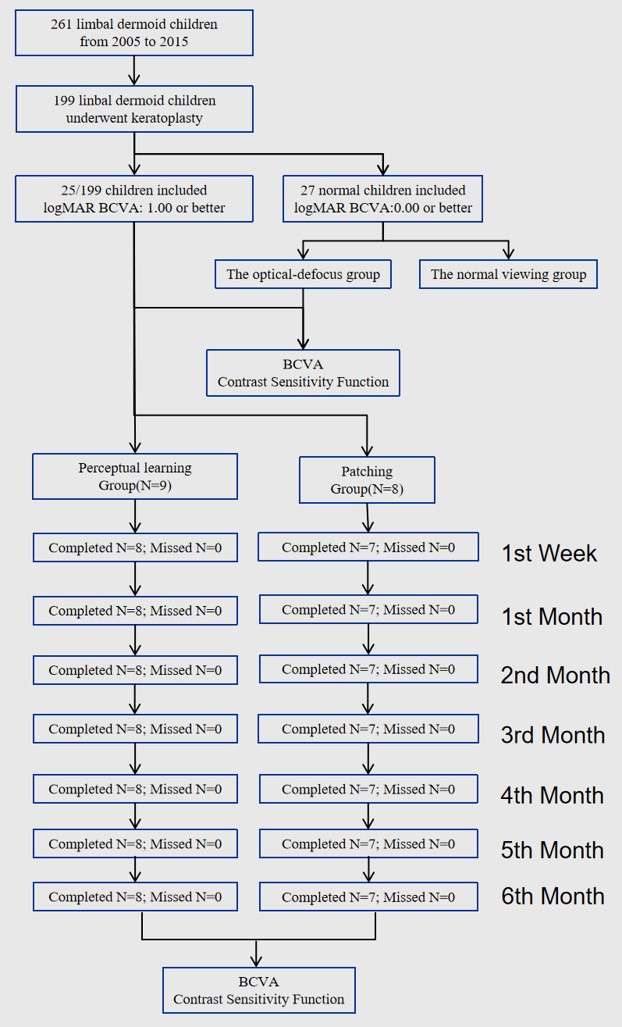
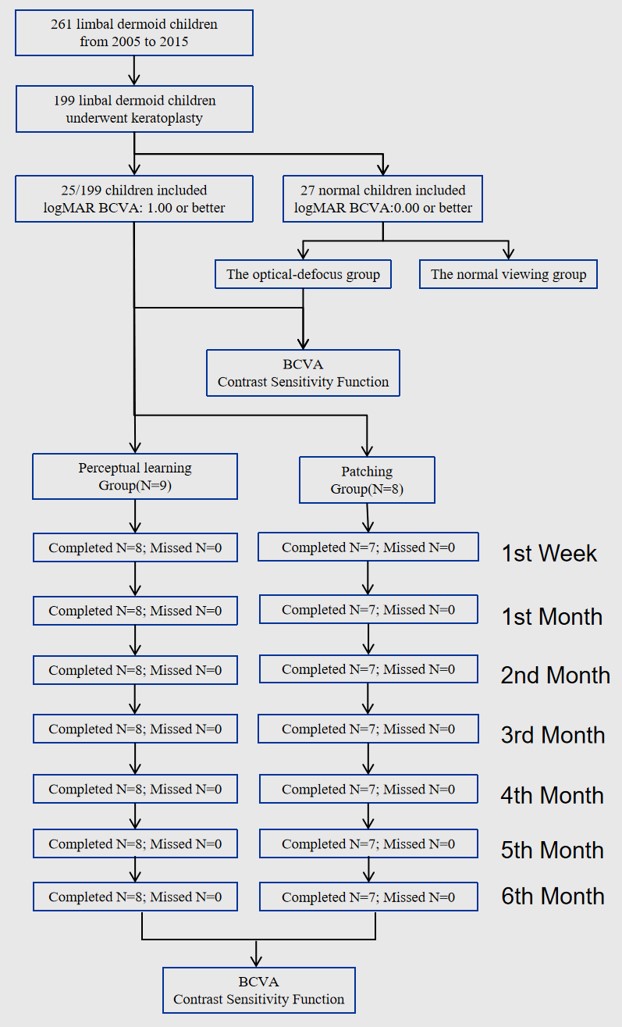
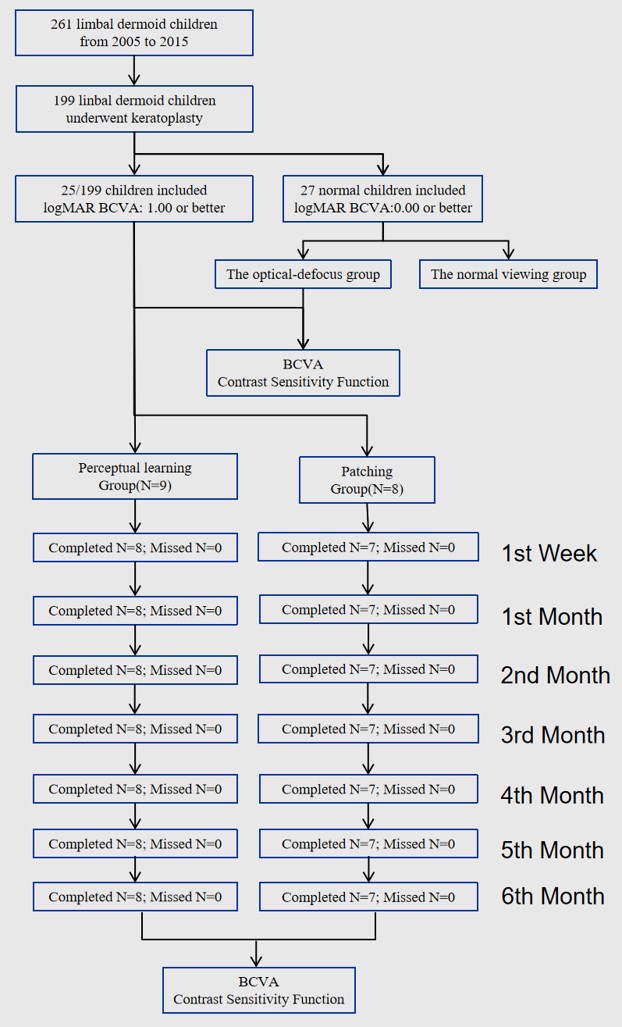
Some experiences have been acquired in our study on perceptual learning for LD children. First, the logMAR BCVA should be at least 1.00 or better to ensure that the children could recognize the visual target clearly, as persistence of the improved visual function showed that learning is not just a temporary adaptation effect but a long-lasting change in the visual cortex [26], and attention plays an important role in selecting what we do (and do not) learn effectively [4]. Then, strict supervision and follow-up visits were significant to ensure learning efficiency and compliance because the learning process was constant and gradual and the interruptions worsened the impression of the visual cortex [27], so statistical significance on visual improvement was not observed until 6 months in our study.
To the best of our knowledge, this is the first perceptual learning study to focus primarily on LD children, and perceptual learning therapy was helpful for improving the CSF as well as VA, which holds promise for treating LD children with amblyopia when conventional treatment fails.
{kind=link}
{kind=link}
{kind=link}