Phase 1 Formulation of a 7-day menu with RS
Developing the menu
Phase 1 includes the methods that address the primary objectives (Figure 1). A 7-day high RS menu was developed using a database that quantified the amount of RS in foods commonly consumed by US adults [1]. In brief, the database was a compilation of 94 peer-reviewed research articles published between 1982 and 2018 that measured the amount of RS in commonly consumed foods in the US. The RS amount in each food in the database was reported with moisture included, not on a dry weight basis, which is how the food would be consumed. The high RS menu was formulated to have a weekly average of ~30g of RS/d, which is based on other clinical trials using RS as a supplement where improvements in glucose homeostasis and/or insulin sensitivity were observed [9, 11, 18].
The energy and nutrient content of the recipes and food items in the high RS menu were analyzed using the Nutrition Data System for Research (NDSR; version 2019, Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN, USA). Recipes and food items were adjusted so the daily energy intake was ~2,000 kcal and the macronutrients fell within the Acceptable Macronutrient Distribution Ranges (45-65% of energy from carbohydrate, 10-35% of energy from protein, and 20-35% of energy from fat) [19].
Preparing the food items
Raw ingredients to prepare the high RS menu were purchased from a single local grocery store using the same brand names (when applicable) throughout the study period. All raw ingredients or products were purchased fresh and stored in the food lab to maintain quality and shelf life. The research team prepared all food items individually using recipes where each ingredient was weighed to the nearest gram. All food items were packaged in plastic food containers according to serving size weight, were labeled (e.g., food ID and date), and stored in a manner that increased RS while maintaining safe food handling practices based on industry recommendations [20].
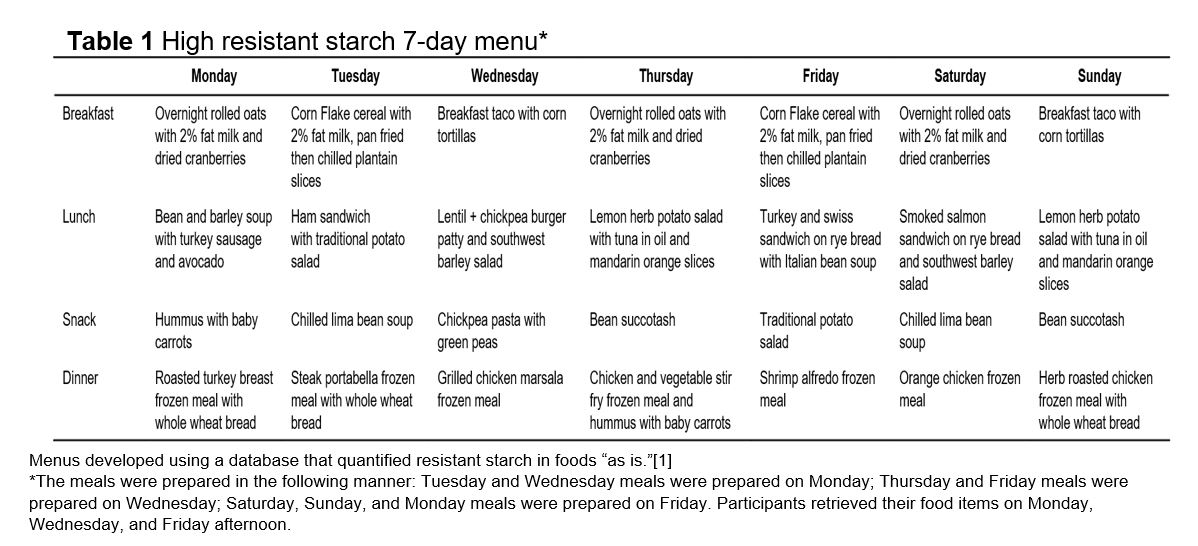
The components each meal is shown in Table 1. The meals were prepared on Monday, Wednesday, and Friday which would be consumed by participants on Tuesday/Wednesday; Thursday/Friday; and Saturday/Sunday/Monday, consecutively.
Analyzing RS content in the menu
RS in foods can be altered due to several factors such as cooking method, storage temperature and duration, and serving temperature [2]. There is a positive correlation between RS formation and duration of cold storage in some cooked, starchy foods [1]. However, in Phase 2 of this study the participants consumed each food item after a minimum of 1 day of storage. Hence RS was analyzed after the food items were stored for 1 day.
Each food item in the menu was prepared twice on separate occasions, and each were analyzed for RS in duplicate. Dry samples or samples with less than 25% moisture such as corn flake cereal, were finely milled for RS analysis. High moisture foods (≥25%) were removed after at least 1 day of storage at 4°C then prepared as would be consumed. For example, rolled oats in milk, plantains, potato salads, sandwiches, and all snack items would be consumed cold; therefore, these items were not heated prior to RS analyses. However, the bean and barley soup, lentil burger, and frozen meals were heated according to instructions and immediately prepared for RS analyses. The rationale for consuming certain items cold but heating other items was to maximize the RS amount in each food item while maintaining food safety and quality. The feasibility of developing, preparing, and storing the 7-day high RS menu was acceptable if the target weekly average of ~30 g RS/d was maintained after one day of storage.
The prepared food items were homogenized, then added to a glass flask filling 1/3 of the container. The flasks were weighed in grams. The food samples were shell-frozen at -80°C for a minimum of 4 hours. Once frozen, the samples were lyophilized for 48-72 hours depending on food sample type. Following lyophilization, the flasks were weighed then moisture content was determined using the following formula: (wet weight (g) – dry weight (g) / wet weight (g))*100.
The dried food samples were finely milled in preparation for RS analysis. All the food samples were analyzed for RS in the prepared form that was “as eaten” according to the Resistant Starch Assay Kit (Rapid) instructions (Megazyme Ltd., Bray, Ireland). The RS measured using this kit employs the AOAC method 2002.02/AACC method 32‐40.01 [21]. The calculations were completed using the Megazyme MegaCalc™ Excel® based calculator provided as supporting documents with the RS analysis kit.
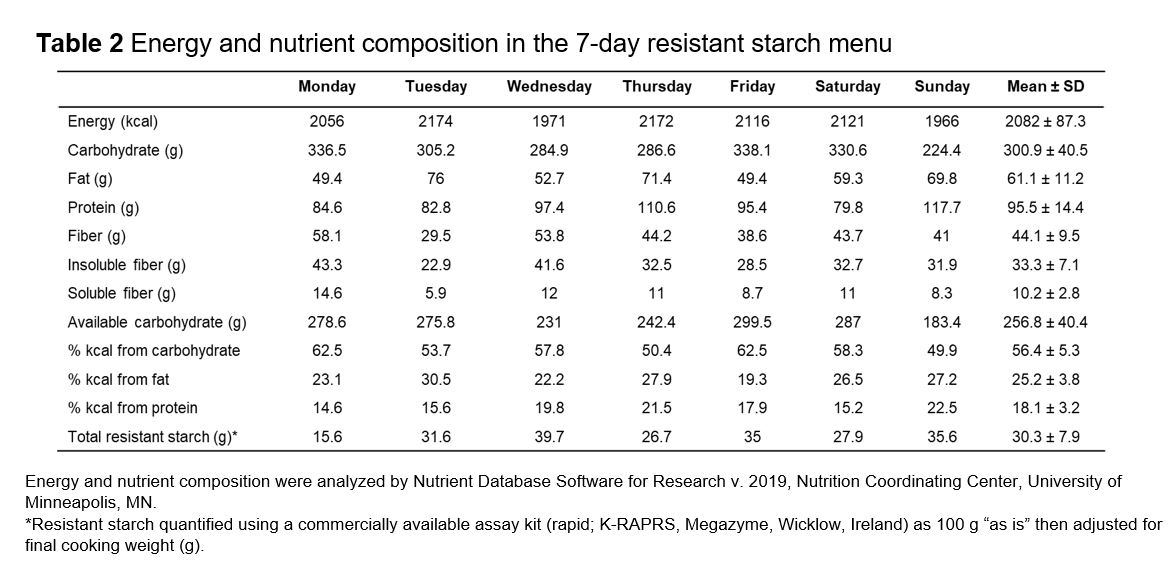
After Initial RS analysis, the recipes and meals were once again slightly adjusted to ensure a weekly RS average of ~30g/d based on RS analysis data and the energy and macronutrient distribution were within the target ranges (Nutrient Database Software for Research, version 2019, Nutrition Coordinating Center, University of Minnesota, MN). Any ready to eat meals or foods that reported low RS was replaced with a food containing high RS (e.g., Chex cereal was replaced by cornflakes). Once the menus were finalized, the RS analyzed in duplicates and mean values were reported as shown in Table 2
Phase 2: Feasibility assessment of menu distribution and evaluation, and changes in anthropometrics and glycemic response
Feasibility of distributing the menu items
The feasibility of distributing the menu to participants was assessed by preparation start and finish times. Feasibility would be accepted if 100% of the food items were prepared, packaged, and distributed to the participants on the same day (second objectives) as shown in the schedule under “Preparing the food items.”
Participants
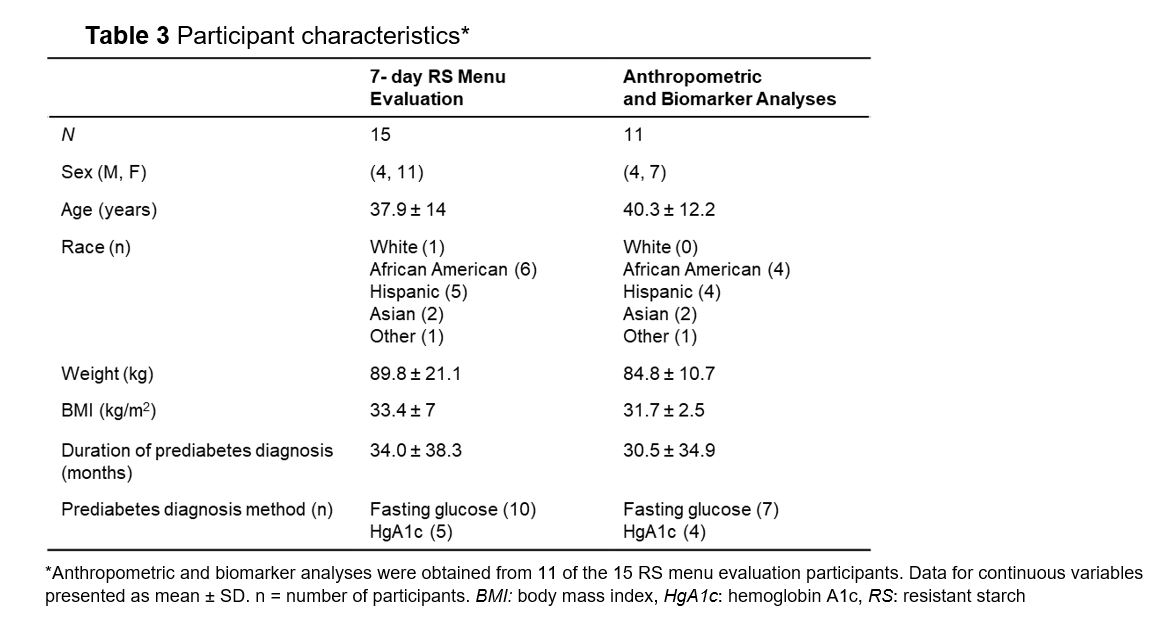
All methods associated with phase 2 addressed the second objectives (Figure 1). First, adults with prediabetes evaluated each menu item (breakfast, lunch, snack, dinner) in the menu containing a weekly average of ~30 g RS/d (first objectives) using a non-randomized dietary intervention. Participants were recruited from the Houston, TX metroplex using flyers, social media, and targeted emails. Interested participants contacted the investigators and were screened for inclusion criteria: adults with a self-report prediabetes diagnosis (e.g., fasting blood 100 – 125 mg/dL, oral glucose tolerance test ≥ 140 - <200 mg/dL, or HgA1c 5.7% - 6.4% mg/dL) [22] from a healthcare provider, between 20 and 65 years of age, able to speak and read English, a BMI ≥27 kg/m2, not following a specific diet or have food allergies or intolerances to any of the study foods, able to safely prepare and consume all study foods. Females were excluded if they were pregnant or lactating. All participants provided written informed consent prior to data collection. This pilot study was approved by the Texas Woman’s University, Houston, TX Institutional Review Board.
Food consumption and evaluation survey
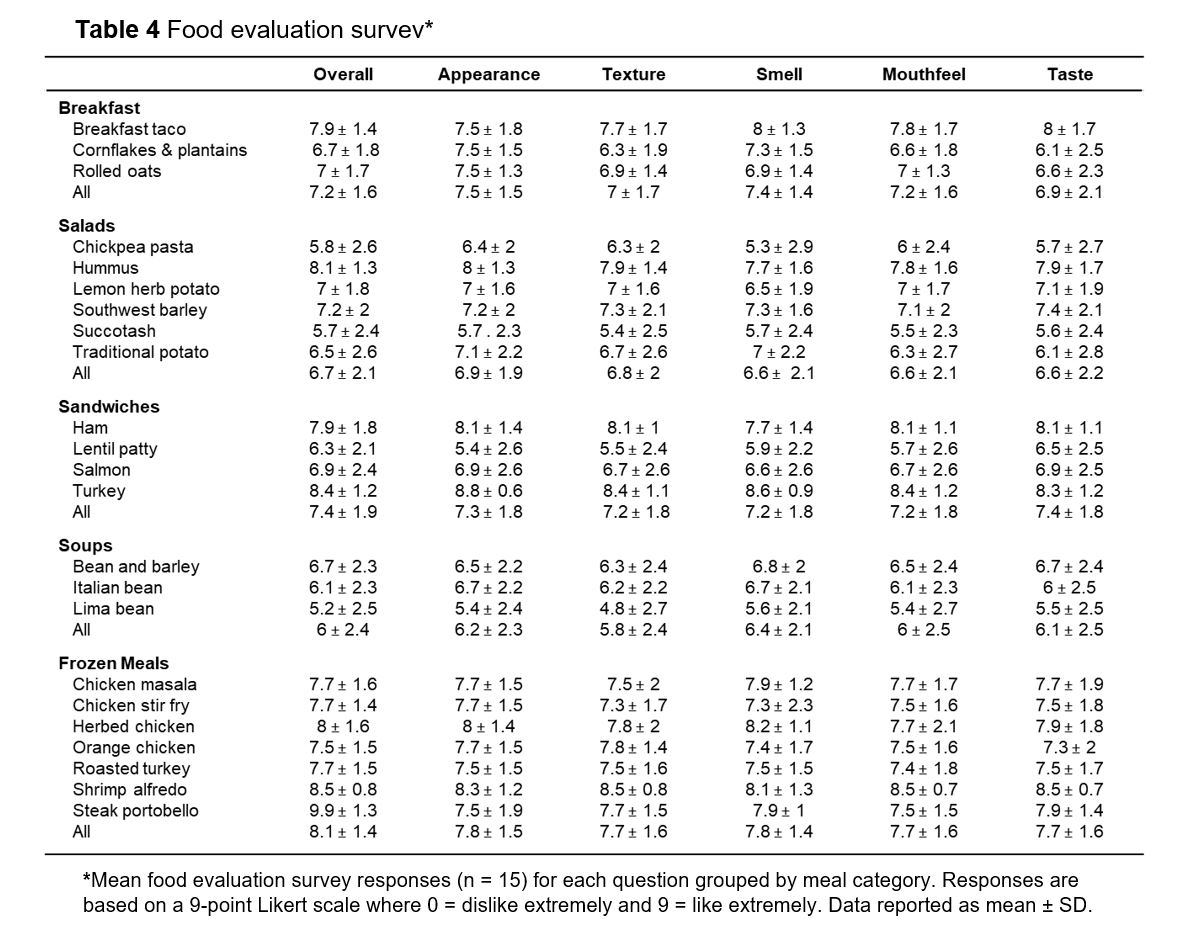
Participants prepared and consumed the food items for each meal and were instructed to avoid consuming additional foods other than non-caloric beverages. Additionally, they received all pre-labeled surveys upon study enrollment. Each breakfast, lunch, snack, and dinner food items were evaluated each day, even if they were consumed more than once during the study. The surveys consisted of six questions that assessed the appearance, texture, smell, consistency or mouthfeel, taste, and overall likeability using a 9-point Likert scale where 1=dislike extremely and 9=like extremely. The survey also contained two open-ended questions regarding what was liked and disliked about the food item and how much they consumed (0%, 25%, 50%, 75%, or 100%). The benchmark established to indicate acceptability for this pilot study was if the participants consumed >75% [23] of the food items in the menu.
The completed surveys were returned to the investigators at the end of the study. To assess the mean response for the question “overall likeability” must be ≥7. Values at or above 7 indicate the food represents sensory characteristics that are acceptable for consumers [23].
Blood analyses
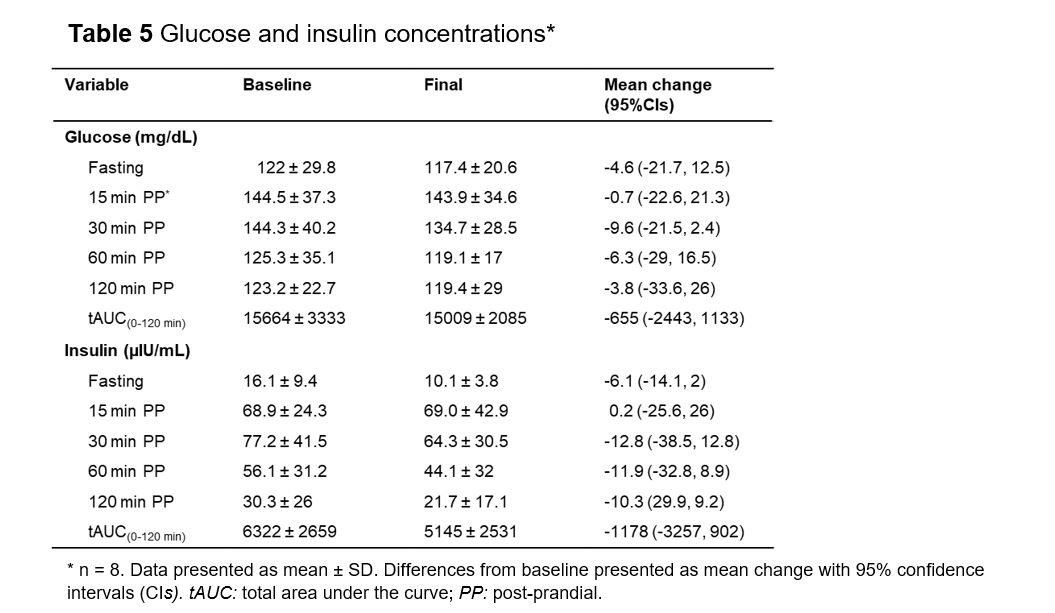
Blood was collected in vacutainers for glucose and insulin analysis. Blood was drawn at fasting (≥8 hours; water allowed) and 15, 30, 60, and 120 min after drinking 360 mL reduced-fat chocolate milk (210 kcal; 19.5g carbohydrate, 6.75g fat, and 6.75g protein) within 10 minutes at baseline (day before beginning RS rich menu evaluation) and the day after consuming the menu. The vacutainers were centrifuged at 4,000 rpm for 10 min and plasma was aliquoted in 1.5 mL tubes and frozen at -80°C until analysis. Glucose was determined using the colorimetric method (Stanbio Laboratory, Boerne, Texas, USA) and insulin by enzyme-linked immunoassay (Alpco, Salem, New Hampshire, USA) according to manufacturer instructions. All samples were analyzed in duplicate and repeated if the intra-coefficient of variation (CV) and inter-CV were ≥10% and 15%, respectively.
Anthropometrics
Height was measured at baseline using a stadiometer. Body weight (kg) was determined at baseline and the day after consuming the 7-day menu using the scale associated with the air-displacement plethysmograph machine (BOD POD, COSMED USA, Inc., Concord, California, USA). Body mass index (BMI; kg/m2) was calculated at each time point. The participants wore the same clothing at both measurements.
Sample size
This pilot study first aimed to evaluate the feasibility of preparing and distributing 7-day menu providing a weekly average of ~30g RS/d in order to investigate potential mechanisms of efficacy for this new intervention. The second objectives tested the likeability of a RS rich menu by human participants. Due to the lack of prior data needed to determine sample size, and the general guidelines for pilot food investigations a sample size of 12 is considered appropriate [24]. Considering this rule of thumb in conjunction with a medium standardized effect size of 0.3 ≤ δ < 0.7 for two time points and one-sided tail with a power of 80%, 15 subjects with prediabetes were considered appropriate to address the second objectives [25].
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences (version 25, IBM SPSS, Armonk, New York, USA). Descriptive data are presented as mean ± SD. All data were screened for normality using Shapiro-Wilk tests and box plots. The tAUC(0-120 min) for glucose and insulin were calculated using the trapezoid formula. Wilcoxon signed rank tests were used to report mean differences and 95% CI for tAUC(0-120 min) glucose and insulin.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}