Patient characteristics
Using the same inclusion and exclusion criteria, we included 7,992 patients admitted from 2001 to 2012 in MIMIC-III database, 8,604 patients admitted from 2014 until 2015 in eICU-CRD database, and 6,730 patients admitted from 2008 to 2019 in MIMIC-IV database (Fig. 1). The baseline characteristics of the patients are shown in Table 1. The majority of patients in the three cohorts were male, and most patients were admitted to the cardiovascular ICU with an initial diagnosis of cardiovascular disease.
Table 1
Baseline characteristics of the study population in the first 24 hours.
| |
MIMIC-III (N = 7992)
|
eICU-CRD (N = 8604)
|
MIMIC-IV (N = 6730)
|
|
Variables
|
Non-AKI
(N = 2158)
|
AKI
(N = 5834)
|
P value
|
Non-AKI
(N = 4105)
|
AKI
(N = 4499)
|
P value
|
Non-AKI
(N = 2000)
|
AKI
(N = 4730)
|
P value
|
|
Age (year)
|
64 (54, 73)
|
69 (60, 78)
|
< 0.001
|
65 (56, 73)
|
69 (60, 77)
|
< 0.001
|
64 (55, 72)
|
68 (59, 76)
|
< 0.001
|
|
Male (%)
|
1421 (65.8)
|
3667 (62.9)
|
0.015
|
2714 (66.1)
|
2760 (61.3)
|
< 0.001
|
1464 (73.2)
|
3177 (67.2)
|
< 0.001
|
|
Body mass index (kg/m2)
|
26 (24, 30)
|
28 (25,32)
|
< 0.001
|
28 (24, 32)
|
29 (25, 34)
|
< 0.001
|
27 (24, 31)
|
29 (25, 33)
|
< 0.001
|
|
White race (%)
|
1551 (71.9)
|
4275 (73.3)
|
0.22
|
3240 (78.9)
|
3532 (78.5)
|
0.65
|
1437 (71.9)
|
3500 (74.0)
|
0.07
|
|
Surgical admission (%)
|
982 (45.5)
|
2454 (42.1)
|
0.006
|
3374 (82.2)
|
3201 (71.1)
|
< 0.001
|
1481 (74.1)
|
3300 (69.8)
|
< 0.001
|
|
Cardiovascular ICU (%)
|
1477 (68.4)
|
4473 (76.7)
|
< 0.001
|
2345 (57.1)
|
2265 (50.3)
|
< 0.001
|
1858 (92.9)
|
4263 (90.1)
|
< 0.001
|
|
History of hypertension (%)
|
1220 (56.5)
|
3702 (63.5)
|
< 0.001
|
2359 (57.5)
|
2803 (62.3)
|
< 0.001
|
1415 (70.8)
|
3608 (76.3)
|
< 0.001
|
|
History of diabetes (%)
|
455 (21.1)
|
1502 (25.7)
|
< 0.001
|
1101 (26.8)
|
1655 (36.8)
|
< 0.001
|
428 (21.4)
|
1052 (22.2)
|
0.47
|
|
History of CKD (%)
|
74 (3.4)
|
580 (9.9)
|
< 0.001
|
192 (4.7)
|
790 (17.6)
|
< 0.001
|
139 (6.9)
|
989 (20.9)
|
< 0.001
|
|
History of CHF (%)
|
436 (20.2)
|
1833 (31.4)
|
< 0.001
|
602 (14.7)
|
839 (18.6)
|
< 0.001
|
345 (17.3)
|
1318 (27.9)
|
< 0.001
|
|
Vasopressor dose (NE, mg)
|
0.2 (0, 2.8)
|
1.8 (0, 7.1)
|
< 0.001
|
0 (0, 0.4)
|
0.1 (0, 4.7)
|
< 0.001
|
0.5 (0, 2.5)
|
1.6 (0.1, 6.1)
|
< 0.001
|
|
Sedatives (%)
|
225 (10.4)
|
718 (12.3)
|
0.023
|
1736 (42.3)
|
1988 (44.2)
|
0.077
|
1602 (80.1)
|
3852 (81.4)
|
0.21
|
|
Mechanical ventilation (%)
|
1763 (81.7)
|
5195 (89.0)
|
< 0.001
|
2875 (70.0)
|
3545 (78.8)
|
< 0.001
|
1935 (96.8)
|
4588 (97.0)
|
0.64
|
|
Transfusion of RBCs (mL)
|
0 (0, 0)
|
0 (0, 0)
|
< 0.001
|
0 (0, 0)
|
0 (0, 0)
|
0.03
|
0 (0, 0)
|
0 (0, 350)
|
< 0.001
|
|
Sepsis (%)
|
1522 (70.5)
|
4370 (74.9)
|
< 0.001
|
1405 (34.2)
|
1805 (40.1)
|
< 0.001
|
1734 (86.7)
|
4137 (87.5)
|
0.41
|
|
Exposure to ≥ 2 nephrotoxins (%)
|
692 (32.1)
|
2084 (35.7)
|
0.003
|
676 (16.5)
|
828 (18.4)
|
0.018
|
578 (28.9)
|
1416 (29.9)
|
0.41
|
|
AKI in the first 24 hours (%)
|
795 (36.8)
|
4447 (76.2)
|
< 0.001
|
715 (17.4)
|
3306 (73.5)
|
< 0.001
|
852 (42.6)
|
3571 (75.5)
|
< 0.001
|
|
Modified SOFA Score
|
3 (1,4)
|
4 (2, 5)
|
< 0.001
|
6 (4, 8)
|
7 (5, 9)
|
< 0.001
|
4 (2, 5)
|
5 (3, 6)
|
< 0.001
|
|
OASISs Score
|
30 (26, 35)
|
33 (28, 38)
|
< 0.001
|
28 (22, 34)
|
31 (25, 37)
|
< 0.001
|
32 (28, 36)
|
35 (30, 40)
|
< 0.001
|
|
TWA-MPP (mmHg)
|
66 (61, 71)
|
62 (58, 67)
|
< 0.001
|
65 (60, 71)
|
62 (56, 68)
|
< 0.001
|
66 (62, 71)
|
63 (58, 67)
|
< 0.001
|
|
TWA-MAP (mmHg)
|
75 (71, 80)
|
73 (69, 78)
|
< 0.001
|
75 (71, 81)
|
73 (68, 79)
|
< 0.001
|
75 (71, 78)
|
73 (69, 77)
|
< 0.001
|
| AKI: acute kidney injury; CHF: chronic heart failure; CKD: chronic kidney disease; ICU: intensive care unit; MAP: mean arterial pressure; MPP: mean perfusion pressure; NE: norepinephrine equivalents; OASIS: Oxford Acute Severity of Illness Score; SOFA: Sequential Organ Failure Assessment; TWA: time weighted-average. |
The median TWA-MPP was 63.1, 63.4, and 63.8 mmHg in MIMIC-III, eICU-CRD, and MIMIC-IV, respectively (Additional file 2: Figure S1). A total of 73.0%, 52.3%, and 70.3% of the study population had recognized AKI in the 24 to 72 hours in three databases. Compared with those without AKI, the patients with AKI were more likely to be elderly, complicated more comorbidities (hypertension, diabetes, chronic kidney disease, chronic heart failure), having a higher rate of AKI in the first day, and higher severity of illness (modified SOFA score and OASIS score), and a higher probability to receive support therapy (vasopressors, mechanical ventilation, and transfusion) in three databases. The patients with AKI also had significantly higher TWA-MPP and TWA-MAP levels as compared to those without AKI. More hospital information, MPP data and outcomes are presented in Additional file 2: Table S1.
Performance of MPP vs MAP for predicting AKI
As MAP was used to represented renal perfusion pressure previously, we compared the performance of MPP versus MAP for predicting the AKI incidence in the next 48 hours (Additional file 1: Figure S2). The results consistently showed that TWA-MPP had significantly larger areas under the curve (AUCs) than TWA-MAP for predicting the incidence of AKI (0.63 vs 0.57, 0.62 vs 0.58, 0.64 vs 0.58 in three databases, all p values < 0.001). TWA-MPP also performed better than TWA-MAP in predicting incidence of AKI using net reclassification index, integrated discrimination improvement, and C statistic (Additional file 1: Table S2) in the fully adjusted models. These findings supported that MPP was superior to MAP as a perfusion predictor of the AKI incidence.
Primary outcomes
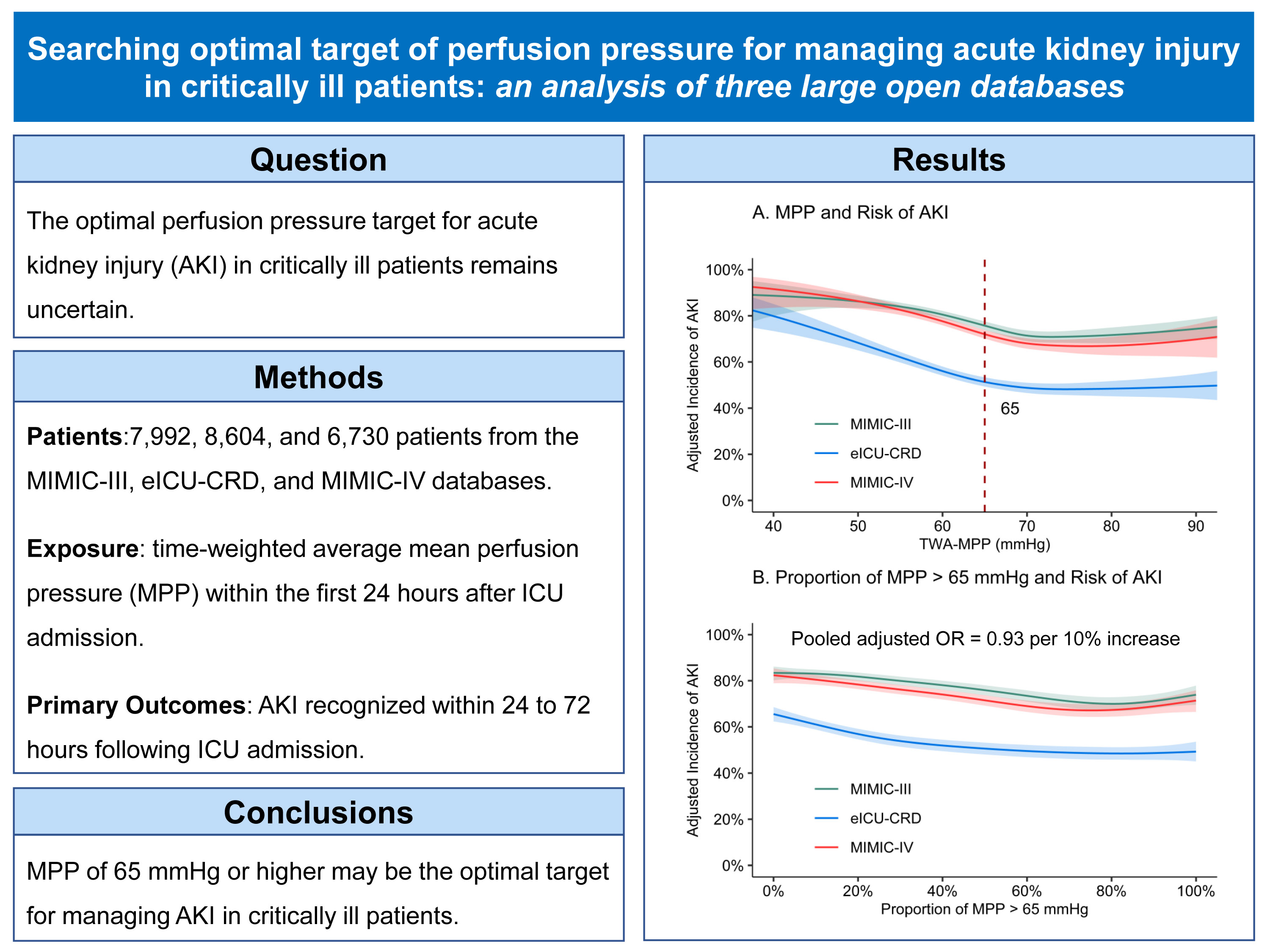
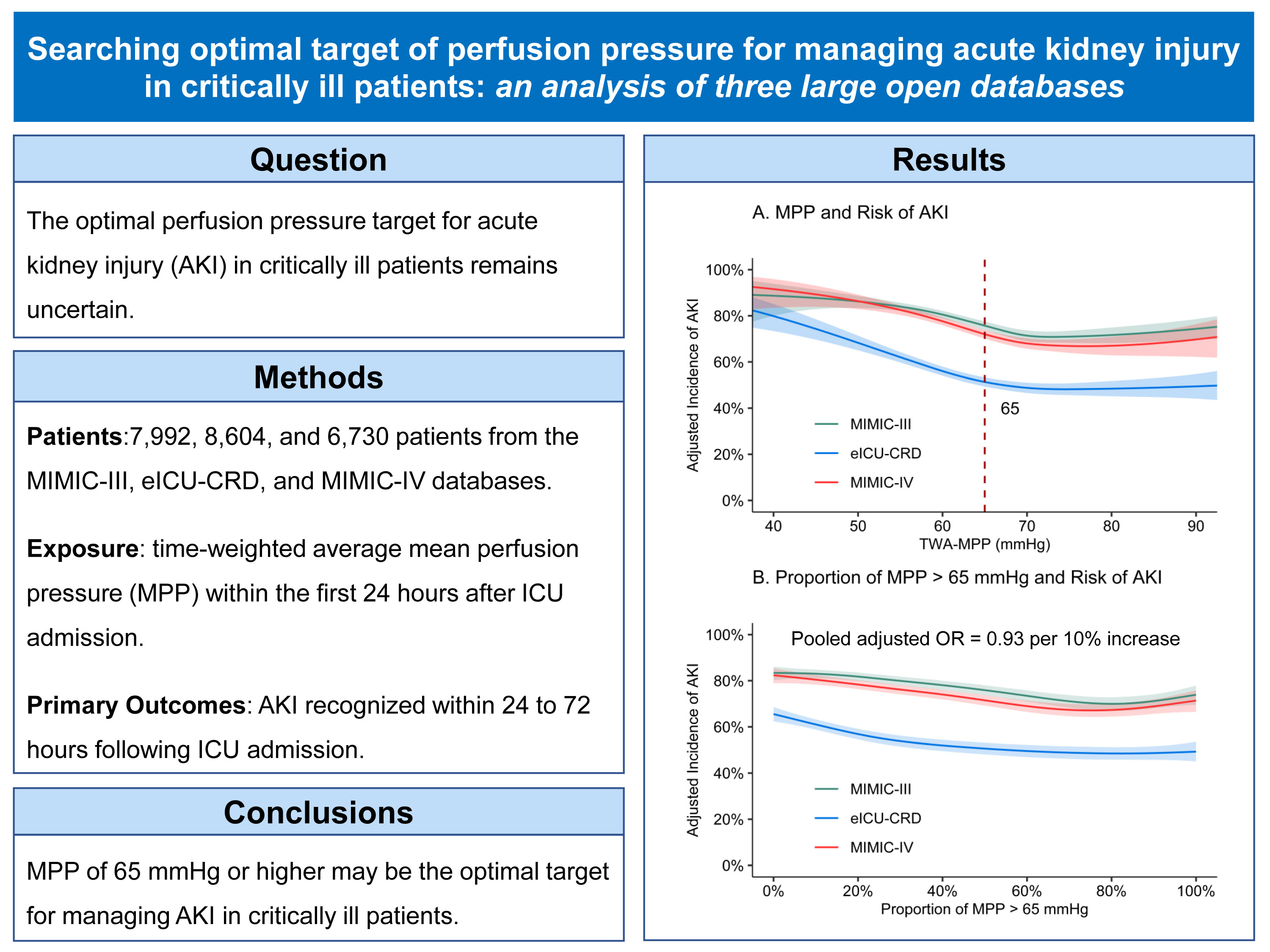
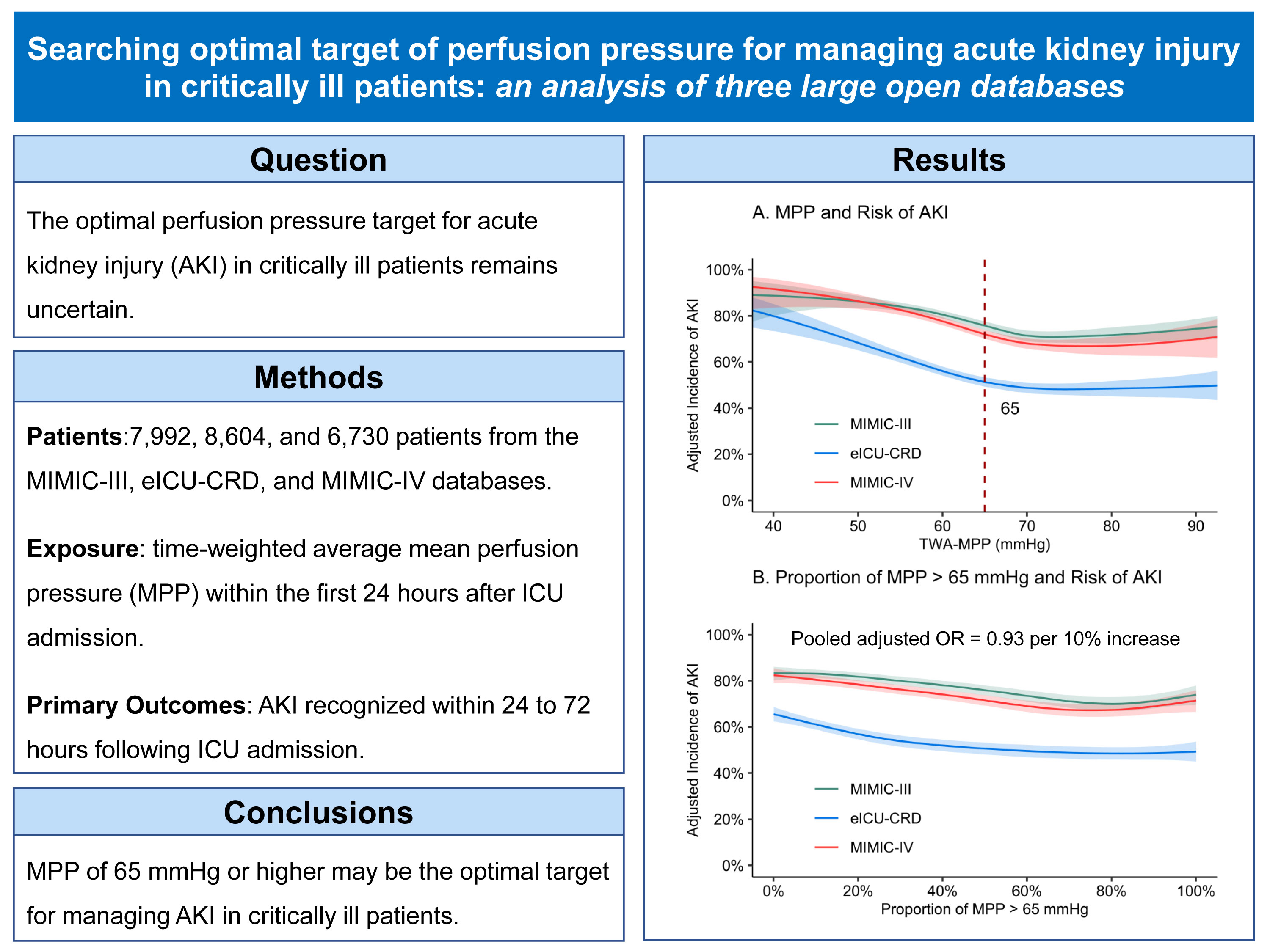
TWA-MPP in the first 24 hours of ICU stay was associated with AKI in the next 48 hours in three databases (Fig. 2A and 2C). We observed the lowest adjusted risk of AKI when TWA-MPP was greater than 72, 65, and 69 mmHg in MIMIC-III, eICU-CRD, and MIMIC-IV, respectively (Table 2). Pooled analyses indicated that per 5 mmHg increase of TWA-MPP below the pooled change point (71 mmHg) was associated with decreased incidence of AKI (pooled AOR = 0.79, 95% CI = 0.76–0.82, p < 0.001).
Table 2
Pooled analyses of estimated change points in the association between TWA-MPP and outcomes from piecewise two-line models.
|
Outcomes
|
No. of Events/Patients
|
Change point (95% CI)
|
AOR per 5 mmHg TWA-MPP increase below the change point (95% CI)
|
AOR per 5 mmHg TWA-MPP increase above the change point (95% CI)
|
|
Primary Outcome
|
|
|
|
|
|
AKI
|
15063/23326
|
71(69–73)
|
0.79(0.76–0.82)
|
1.07(1.02–1.12)
|
|
In MIMIC-III
|
5834/7992
|
72(68–75)
|
0.78(0.73–0.82)
|
1.09(1.00-1.19)
|
|
In eICU-CRD
|
4499/8604
|
65(62–68)
|
0.75(0.70–0.81)
|
1.00(0.95–1.06)
|
|
In MIMIC-IV
|
4730/6730
|
69(66–72)
|
0.73(0.67–0.79)
|
1.05(0.94–1.16)
|
|
Secondary Outcomes
|
|
|
|
|
|
Severe AKI
|
9767/23326
|
70(68–72)
|
0.81(0.79–0.84)
|
1.08(1.03–1.14)
|
|
New-onset of AKI
|
3351/8213
|
74(70–78)
|
0.83(0.79–0.87)
|
1.08(0.98–1.18)
|
|
Persistence of AKI
|
10283/12266
|
70(68–72)
|
0.76(0.72–0.80)
|
1.12(1.04–1.22)
|
|
Progression of AKI
|
2949/12266
|
65(60–71)
|
0.88(0.84–0.93)
|
1.00(0.95–1.06)
|
| The table shows that the lowest probability of incidence of AKI and severe AKI, new-onset, persistence, and progression of AKI was observed when TWA-MPP below a change point. The lowest of these change points was 65 mmHg. Thus, our findings support an optimal target of 65 mmHg or higher in MPP for the management of AKI. Adjusted factors included the top 19 factors listed in Table 1. |
As eICU-CRD database represented multicenter and recent practice after publishing the 2012 Kidney Disease: Improving Global Outcomes AKI guideline, and 65 mmHg was the lowest change point of MPP for the incidence of AKI in the three database, we chose MPP of 65 mmHg as a conservative perfusion pressure target for the management of AKI. We furtherly found that the increase in the proportion of MPP > 65 mmHg was associated with less incidence of AKI in unadjusted and adjusted analyses in three databases (Fig. 2B and 2D). Pooled analyses indicated that per 10% increase of proportion of MPP above 65 mmHg was associated with decreased incidence of AKI (pooled AOR = 0.93, 95% CI = 0.92–0.94, p < 0.001).
Secondary outcomes
TWA-MPP in the first 24 hours of ICU stay was associated with new-onset, persistence, and progression of AKI in the next 48 hours in the three databases (Fig. 3, Additional file 2: Table S3). The pooled analyses indicated that a lowest probability of new-onset, persistence, and progression of AKI were estimated when TWA-MPP above 74, 70, 65 mmHg, respectively (Table 2). Per 5 mmHg increase in TWA-MPP below these change points was associated with a lower probability of new-onset (pooled AOR = 0.84, 95% CI = 0.80–0.87, p < 0.001), persistence (pooled AOR = 0.76, 95% CI = 0.72–0.80, p < 0.001) and progression (pooled AOR = 0.88, 95% CI = 0.84–0.93, p < 0.001) of AKI.
Sensitivity and subgroup analyses
First, the change points of MPP were in the range of > 65 mmHg in critically ill patients who received vasopressors during the first 24 hours (Additional file 2: Figure S3, Additional file 2: Table S4). Second, the optimal target of MPP did not shift when median MPP was included into the analyses instead of TWA-MPP (Additional file 2: Figure S4, Additional file 2: Table S5). Third, the different definitions of baseline creatinine determined by the nadir creatine during 7 days before and after ICU admission did not totally affect the association between TWA-MPP and the AKI incidence (Additional file 2: Figure S5, Additional file 2: Table S6).
The association of TWA-MPP and the AKI incidence was analyzed across patients who with or without elderly (≥ 65) and hypertension, diabetes, chronic kidney disease, sepsis, vasopressor-treated, higher above median SOFA score at the first day of ICU admission (Fig. 4). The subgroup analyses consistently support the MPP of 65 mmHg or higher in the management of AKI.
{kind=link}
{kind=link}
{kind=link}