To our understanding, this is the first study that assesses the incidence of new-onset pain and its influence on the quality of life in critical illness survivor in one specific disease.
We found that half of the critical illness covid-19 survivors report new pain in the first month after hospital discharge, it was frequently associated to a significant worse quality of life.
The few studies that evaluate new-onset pain in intensive care survivors have been carried out in mixed surgical and medical ICUs, reporting an incidence between 18% and 44%, depending on the study population, the tool used to assess pain and the time of measurement. (Battle et al, 21; Baumbach et al, NEW BIBLIOGRAPHY (PMID: 26958751; Kroster-Brauwer et al, 22). Although we did our evaluation in a shorter period of time than the studies discussed above, we believe it is important to report these findings to the medical community, so actions can be taken to improve outcomes for these patients.
Characteristics of pain
Interestingly, one third of the patients suffering from new onset pain had a positive screening for neuropathic pain. Human coronavirus are neurotropic and potentially neurovirulent viruses[20]. It is widely known the association of acute and chronic neuroinflammation with various neurological process[21]. COVID-19 is capable of triggering a cytokine storm in specific populations, with immediate, but also probably lasting effects, on the central and peripheral nervous system[20]. Although there are no conclusive data about the possible persistence of neuroinflammation in survivors of COVID-19 disease, neuropathic pain could be a manifestation of this process that needs to be further investigated.
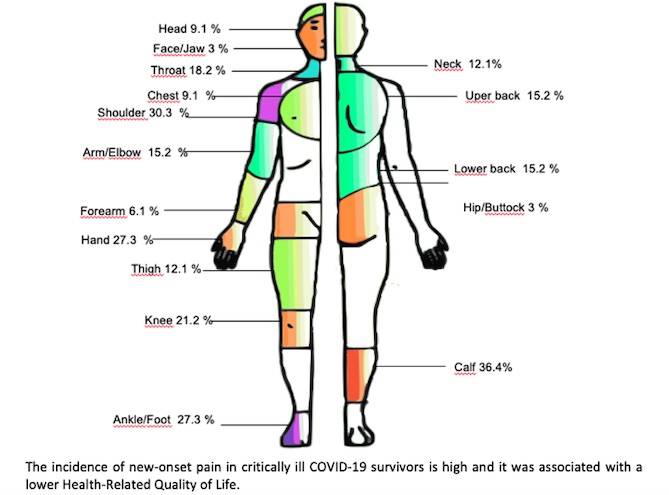
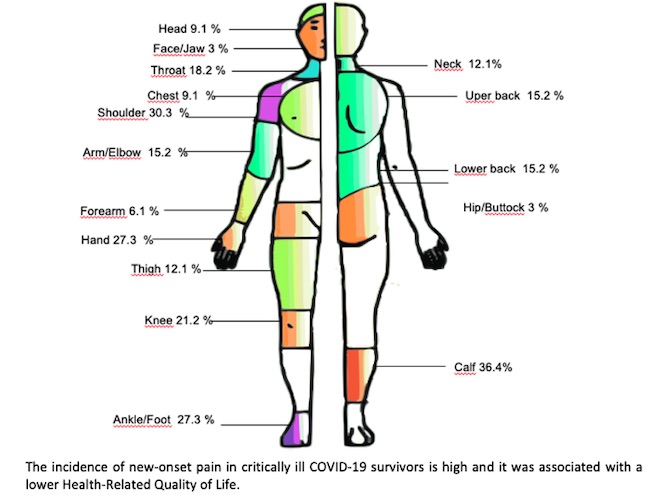
As it has been observed in previous studies in critical illness survivors, the majority of patients reported pain in multiple body areas, being bilateral symptoms common. Similarly, shoulder pain is also frequently reported[22]. The shoulder joint is vulnerable due to multiple factors such as the relationship of muscle atrophy resulting after relaxation, corticosteroid therapy, sedation and mechanical ventilation [23][20][28]. Other possible causes are invasive devices such as central venous line or dialysis catheter placed in this area[22] or different maneuvers used to move the patients which often depend on the pressure exerted on this joint.[21]. Brachial plexus injury during prone positioning mechanical ventilation has been identified as another potential cause during the pandemic.[24] Therefore, a call has been made for a protocolization of safe proning procedures and an active identification of pain and functional limitation after extubation of the patient[25]. Our results also highlights that 15.2% of the patients with pain presented widespread pain. A chronic post severe acute respiratory syndrome has been described, as a fibromyalgia-like syndrome[26], in which neuroinflammation would explain this symptomatology. To establish this fact, it would be necessary to demonstrate generalized hyperalgesia (suggesting central sensitization) by means of a quantitative sensory test that should be performed in subsequent studies[27].
Anxiety and depression
We found a lower prevalence of anxiety and depression in this population (HAD anxiety 10.8%, HAD depression 7.7%) than in previously reported non-COVID-19 critically ill patients where it has been documented as high as 46% and 40% for anxiety and depression, respectively at 3 months.[28]
Davydow et al. [29] also observed that the median point prevalence of clinically significant depressive symptoms among ICU survivors was 28% (range 8–57%) 2 months after hospital discharge. In this systematic review, described a potential for selection bias, due to the voluntary participation. The authors speculated that patients with more severe PICS may refuse to participate in the study due to mood disturbances. However, the median point prevalence of clinically significant depressive symptoms described by Davydow et al [29] was 28%, higher than what we found.
Alternatively, the patients could develop a posttraumatic growth, defined as positive changes that a person can experience as a result of struggling with trauma [30]. The so called Polyanna Syndrome, described as being "blind optimistic" to a bad situation[31], could also explain the unexpected low incidence of depression given the survival of to the pandemic.
HRQoL
Up to 69% of patients displayed some kind of difficulty for mobility in the EQoL-5D/5L questionnaire, whereas the least affected dimension was self–care in 30.8% of patients Even if many patients were affected in one or more dimension of EQoL-5D/5L, the EQoL-5D/5L VAS evidenced that they had a better perception of their health status than expected, which could be related to the feeling of being a survivor of the pandemic but when the EQoL-5D/5L dimensions are analyzed, the alterations are objectified.
Correlation and clinically significant pain
The intensity of pain measured with BPI-SF was negatively correlated to both EQoL-5D/5L VAS and EQoL-5D/5L index value. This correlation has been described for many pathologies and usually related to an injury as a trigger of pain[32]. The EQoL-5D/5L index value and therefore, the reported HRQoL, was lower in those patients who reported a greater intensity of pain. As far as we know, this is the first study showing the association of clinically significant pain and HRQoL on any type of PICS patients, either COVID-19 or non-COVIID-19 patients. Whether our findings will remain stable over time is not known at this point. However, this research sheds light on the importance of better characterizing physical and mental trajectories after ICU admission to offer best long-term patient care.
{kind=link}
{kind=link}