Basic facts
The group includes 20 male patients and 12 female ones in the age bracket of 16-45 years old (31.1±8.6). All the cases are acute injuries, with 18 injured on the left knee and 14 on the right knee, and their hospital stay lasted 5-23 days (13.6±5.8). There were various causes behind injuries: 10 cases were injured in traffic accidents, 10 were injured by falls, 7 were sprained from sports, and 5 were injured by heavy objects.
Inclusion Criteria: confirmed ACL injury (alone or concurrent with meniscus injury; Fig1), aged 16-45 years old and having complete follow-up data available. Exclusion Criteria: concurrent with a ruptured posterior cruciate ligament, medial and lateral collateral ligament or patellar support belt, injured cartilage tissues, fractures around the knee joint, and/or a diseased lower limb and/or an abnormal contralateral knee joint; more than 1 year after the surgery; concurrent with severe skeletal, muscular or neurological diseases on the ipsilateral limb, such as osteoarthritis, femoral head necrosis, tuberculosis, lumbar disc herniation, diabetic foot,etc; and the history of cerebral infarction and/or abnormal strength of lower limb muscles.
Surgical Method
All operations were performed by the same surgeon, and the endobutton and BioRCI interface screws from Smith & Nephew were used as the locking screws in these operations. The patients under general anesthesia were lying on the supine position, with balloon tourniquets wrapping around the upper third of their thighs, and the anterolateral and anteromedial approaches for arthroscopic surgery were established. The arthroscopy was then inserted from the anterolateral entrance and careful checks were made to confirm ACL raptures.
PLT preparation: firstly, make an about-3-cm-long longitudinal incision on the affected limb at the position 1 cm away behind and 2-3 cm over the lateral malleolus (the incision should not be too far away to prevent the possible friction between the incision scar and the upper shoe edge in future) for exposing and separating the PLT and the PBT in order; next, cut off the distal end of the PLT; then, carefully peel off the proximal end of the PLT with a key extractor; further then, cut off the proximal end at the point 4-5cm away from the fibular head and weave the removed PLT into a double bundle; and finally, under arthroscopy, strip the remaining ACL off from the synovial membranes and fatty tissues at the femoral attachment point, clean off its stump and keep it. Do be careful all the way to prevent any damage to the common peroneal nerve.
Tibial Tract Fabrication: the tibial tract is about 45-50 mm in length (consisting of the lengths of the graft and the femoral tract and the intra-articular distance), about 8 mm in diameter and opens at the intersection of the extension line of the lateral meniscus and the intercondylar ridge, about 7 mm away in front of the PCL.
Correctly adjust the position and angle of the positioner, insert the guide needle, confirm that the entry point is at the right position, and select a suitable drill for fabricating the tibial osseous canal. The femoral bone canal is fabricated in the following process: firstly, have the knee joint flexed at least 70 degrees, insert the guide wire backward through the tibial canal deeply till reaching the marked opening on the femoral osseous canal (located inferoposterior to the angulation point between the resident ridge - a bony landmark for arthroscopic femur localization - and the interfacial ridge); next, have the drill bit pass through the guide needle and the tibial bone canal till touching the back of the femoral wall, with the penetration depth of the drill bit being about 25-30 mm; then, lead the prepared tendon out through the bone canals of the tibia and femur with a traction line, and fix the femur with a looped plate and the tibia with a bioabsorbable screw; further then, check the position and stability of the graft under arthroscopy, and conduct drawer tests while flexing and extending the joint; and finally, suture the incision after confirming no dysfunctions, apply elastic bandage on the incision and support the limb with a brace. After the operation, perform MRI and CT three-dimensional reconstruction examination on the patient's surgical site. (Fig2-3)
Postoperative Treatment and Rehabilitation
Keep the postoperative knee joint in the compression bandaging for five days for reducing the swelling and fully extended and fixed with a brace for 4 weeks; do isometric exercises of quadriceps and exercises of straight leg lifting 2 weeks later; do protective ROM exercises under partial load and in the range of motion from 0 to 90 degree 4 weeks later; do ROM exercises under full load and in the range of motion from 90 degrees to full extension 8 weeks later; perform daily activities, stand on one leg or do exercises with a stationary bicycle 5 months later; do light-intensity physical exercises 6 months later; do continuous jump tests 12 months later; and resume normal physical exercises (if the continuous jump tests show a satisfactory results).
Evaluation Indicators and Statistical Methods
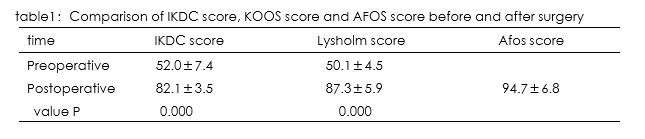
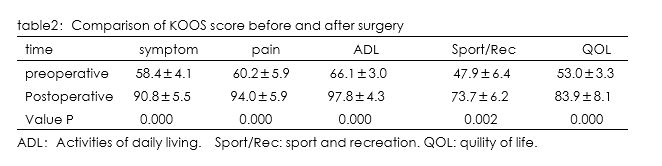
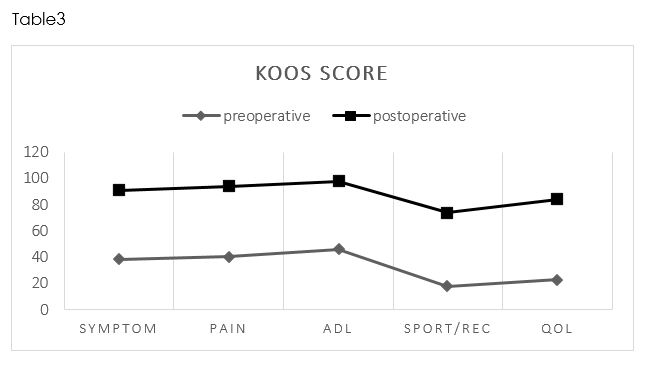
IKDC score, KOOS score, Lysholm score were used for evaluating the knee joint function of the affected side, AOFAS score for evaluating the ankle joint function of the donor site, and SPSS 20 statistical software for analyzing the collected data of each group in the form of mean ± standard deviation. First, check the normality of data of each group through Shapiro-Wilk tests, finding that the scores of each group before and one year after the operation did not conform to the normal distribution (P<0.1); then, check the normality of the difference between the data of each group before and after the operation, finding that the difference conformed to the normal distribution (P>0.1); and finally, compare and analyze the scores before and after the operation through paired t tests, with the test level being α=0.05.
{kind=link}
{kind=link}
{kind=link}