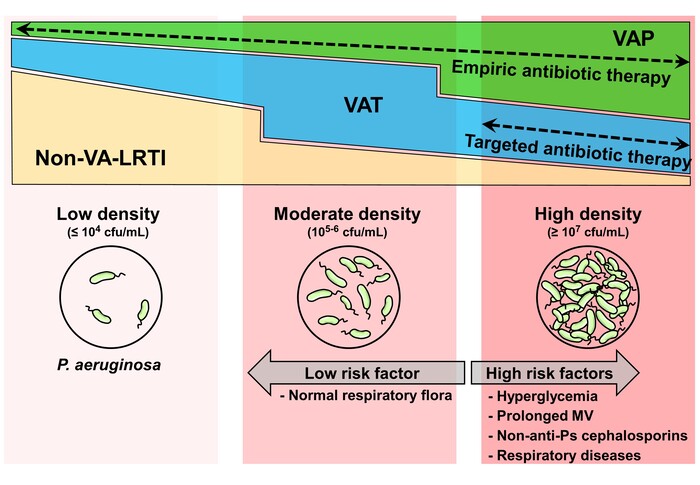
In this study, we investigated the relationship between airway PA density and clinical outcomes in MV patients, as well as the effects of antibiotic treatment. To the best of our knowledge, no previous study has highlighted the importance of airway PA density in MV patients or identified the risk factors for high PA. We found that high-PA was associated with worse clinical outcomes. Prolonged MV, non-antipseudomonal cephalosporins, hyperglycemia, and respiratory diseases were associated with higher risk, whereas the presence of commensal colonizers was associated with a lower risk for high-PA. Moreover, AAT for VAT patients was related to improved weaning from MV, but only in the high-PA group.
The relationship between airway PA density and clinical course has been reported for various respiratory diseases. A previous analysis of 385 patients with bronchiectasis showed that bacterial density was directly correlated with airway and systemic inflammatory markers, such as myeloperoxidase activity, neutrophil elastase activity, and tumor necrosis factor-α levels [30]. Airway bacterial density was also associated with exacerbation frequency and health-related quality of life. We found that MV patients with high-PA had more severe airway (neutrophils in the ETA) and systemic inflammation. CRP levels were lower in the moderate-density group than in the other groups, which may be due to underlying hepatobiliary diseases that were slightly more frequent in the moderate-density group (26.9% in the moderate group vs. 19.9% in the other groups), affecting CRP production. The frequency of VA-LRTI was low in the low-PA group, while the high-PA group had more cases of VAP than other groups. Patients with high-PA may develop more severe respiratory infections, reflecting the higher inflammatory response in cases with high bacterial density. Our study found that the high-PA group had prolonged weaning from MV and higher ICU mortality. These results were similar when adjusted for the severity scores by multivariate analysis. Thus, the pathogenicity of PA, particularly when present at a high density in the airway, is expected to have a significant impact on the inflammatory response and the clinical course in MV patients. On the other hand, a recent study did not detect an association between bacterial density and progression to VAP in critically injured ventilated patients [31]. However, comparisons by pathogen species were not made in their study. The host immune response varies greatly depending on the type of pathogen [32–34], and the relationship between bacterial density and clinical outcomes in MV patients seen in our study may be different for pathogens other than PA. The relationship between colonization and progression to infection is not solely determined by bacterial density; the host immune status is also an important factor. Currently, potential markers such as volatile organic compounds [35], soluble triggering receptor expressed on myeloid cells 1 [36], and pentraxin 3 [37] are expected to be used for early diagnosis of VAP. Further research based on a comprehensive evaluation that includes these factors, as well as the bacterial burden, is needed to better understand respiratory infections in MV patients and to further optimize antibiotic use.
PA was isolated from ETA in 18% of ICU patients for surveillance and clinical cultures at our institution during the study period. The isolation rate of PA from ETA in previous reports varied from 5.8% to 27.9% [38, 39], and the decision which of these patients should be treated with antibiotics is an important issue in daily practice, particularly for patients with VAT, as an intermediate stage between airway colonization and VAP. The first randomized controlled trial of treatment for VAT demonstrated that patients who received AAT had higher numbers of VFD (median 12 vs. 2 days) and lower ICU mortality (18% vs. 47%) than the no antibiotic group [40]. Another randomized controlled trial showed that inhaled antibiotics in patients with VAT reduced symptoms of respiratory infections and increased weaning [41], and recent multicenter observational studies reported that appropriate antibiotic therapy reduced the progression of VAT to VAP [42, 43]. On the other hand, several studies reported no significant benefit of AAT [44, 45]. One of the problems with VA-LRTI studies is that although the diagnostic criteria for VAT and VAP are almost similar in each study, the interpretation of chest X-ray in the ICU may be affected by various artifacts and diseases other than pneumonia, sometimes making it difficult in practice to differentiate between VAT and VAP [46]. Other problems include differences in causative bacteria and antibiotic regimens used across studies. A recent guideline does not recommend routine use of antibiotics for VAT, given the inconsistent evidence of clinical benefit and the problem of adverse drug events [47]. The guideline suggests assessing the condition of individual patients and considering antibiotic therapy depending on disease severity. However, it is not yet known in which subgroups antibiotic therapy is particularly effective for VAT. In the present study, the number of airway neutrophils in VAT patients with high-PA was higher than that in other groups, suggesting that antibiotics may be particularly effective in these patients. Indeed, in our propensity score-matched analysis, AAT improved MV weaning outcomes only in VAT patients with high-PA. This relationship between PA density and the therapeutic effect of antibiotics was also supported by a recent study of patients with bronchiectasis [48].
We also explored the risk factors associated with high-PA and identified five significant variables: respiratory diseases at ICU admission, prolonged MV (> 28 days), non-antipseudomonal cephalosporins, hyperglycemia, and commensal colonizers during ICU stay. Respiratory diseases, duration of MV, and ineffective antibiotics against PA are well-known risk factors for PA colonization and infection in MV patients [23–25]. We newly identified hyperglycemia as an important risk factor for high-PA. In vitro and animal experiments showed that, as the blood glucose increased, the glucose concentration in the airway surface liquid also increased, which promotes the growth of airway PA and causes severe pneumonia [49, 50]. In human trials, airway glucose concentration was affected by blood glucose level and the presence of respiratory disease. Critically ill patients receiving MV showed high airway glucose levels [51]. For these reasons, the airways of MV patients with hyperglycemia may provide a more favorable environment for PA growth. We also found that isolation of commensal colonizers during the ICU stay was associated with a lower risk of high-PA. Bacteria have complex effects on each other. For example, Candida spp. downregulate quorum sensing of PA by farnesol [52], whereas oral commensal Streptococcus spp. suppress the growth of PA by producing hydrogen peroxide [53]. Thus, commensal colonizers may have protective effects against the growth of PA.
Our study had several limitations. First, as it was a retrospective analysis from a single ICU, our findings are subject to bias and may not be generalizable to all ICU patients. Second, 27.1% of our patients had been exposed to anti-pseudomonal antibiotics at the time of collecting the ETA sample, which may have affected the density of the isolated PA. However, the proportion of patients receiving anti-pseudomonal antibiotics was comparable among the three groups. Similarly, 29% of the samples in which the peak density of PA was detected had pathogens other than PA. Although the number of pathogens with a high bacterial density of 105 cfu/mL or more was small in all cases (< 7.4%), bacteria have a complex relationship with each other, and these effects could not be completely ruled out in this study. Moreover, we could not evaluate respiratory infections caused by bacteria other than PA. Since these affect the length of MV, they may also have some effect on the peak density of PA. Third, we were unable to evaluate antibiotic therapy in detail, including the regimens and lengths of administration, due to the small number of patients. The major limitation of this study was the long study period. Our clinical practices in ICU changed during the study period. For example, a VAP prevention bundle involving a semi-recumbent position, as well as the daily assessment of sedation and extubation readiness, was initiated in 2010. With the revision of the guidelines, therapeutic policies regarding antibiotic regimens and duration of VAP treatment were also changed, and optional treatments such as adjunctive macrolide use and inhaled antibiotics were adopted. Microbial changes in ICU were also observed, the prevalence of MRSA decreased, that of Haemophilus spp. increased, and that of PA did not change during this study period. The ratio of patients selected from the first half of the study period to those selected from the second half was similar in each PA density group; however, we were not able to assess the impact of these changes in clinical practice on the results. This is an important limitation of this study, and further research is required to understand the effects of bacterial density in MV patients.
{kind=link}