Study population
This study was approved by the Biomedical Research Ethics Committee of our hospital and conducted in accordance with the Declaration of Helsinki (2013 Edition). Due to the retrospective nature of the research, the need for informed consent was waived.
This research included 255 individuals with T2DM who were clinically diagnosed based on the current American Diabetes Association guidelines and who underwent CMR examinations at our hospital between April 2012 and April 2021 [12]. The exclusion criteria were patients with a history of primary cardiomyopathy, congenital heart disease, myocardial infarction, rheumatic heart disease, estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2, or other severe non-AR valve regurgitation diseases and those with a poor image quality for post-processing analysis. Finally, 215 patients who met these criteria were included in the analysis and were categorized into two groups according to the presence or absence of AR: those with T2DM but without AR (T2DM [AR-]) (n = 149) and those with T2DM who presented with AR (T2DM [AR+]) (n = 66). The diagnosis of AR and regurgitant degree were based on echocardiography (Additional file 1). The average age and body mass index (BMI) of patients with diabetes were 54 (range: 48–60) years and 22.96 (range: 21.03–26.00) kg/m2, respectively. Among them, 66 (37.6%) presented with AR (n = 28, mild; n = 21, moderate; and n = 17, severe), whereas 149 (62.4%) did not. Concurrently, 83 individuals with sex, age, and BMI distribution similar to those of our patients were included in the control group. All patients and controls underwent the same CMR examination.
Basic information and laboratory data collection
Data regarding age, sex, disease duration, blood pressure, height, and weight were extracted, and BMI was calculated. In addition, we collected the following laboratory and clinical data: fasting blood glucose, glycated hemoglobin, triglyceride, total cholesterol, high-density lipoprotein and low-density lipoprotein cholesterol levels, duration of diabetes (years), and use of antidiabetic drugs (α-glucosidase inhibitors, biguanides, sulfonylureas, glucagon-like peptide-1/dipeptidyl peptidase-4 inhibitors, sodium-glucose cotransporter 2 inhibitors, and insulin). The baseline information of healthy controls was collected before CMR scanning.
CMR protocol
A 3.0-T whole-body scanner (Skyra; Siemens Medical Solutions, Erlangen, Germany) with a 32-channel body phased-array coil was used to examine patients while in the supine position. Data were acquired during the breath-holding period at the end of inspiration. A series of 8–12 consequent short-axis views of the LV from the aortic valve to the level of the LV apex were obtained using steady-state free precession with the following parameters: temporal resolution, 39.34 ms; echo time, 1.22 ms; slice thickness, 8.0 mm; flip angle, 39; field of view, 234 × 280 mm2; 1.31 ms; and matrix size, 208 × 139 pixels.
Image analysis
Calculation of LV volume and functional parameters
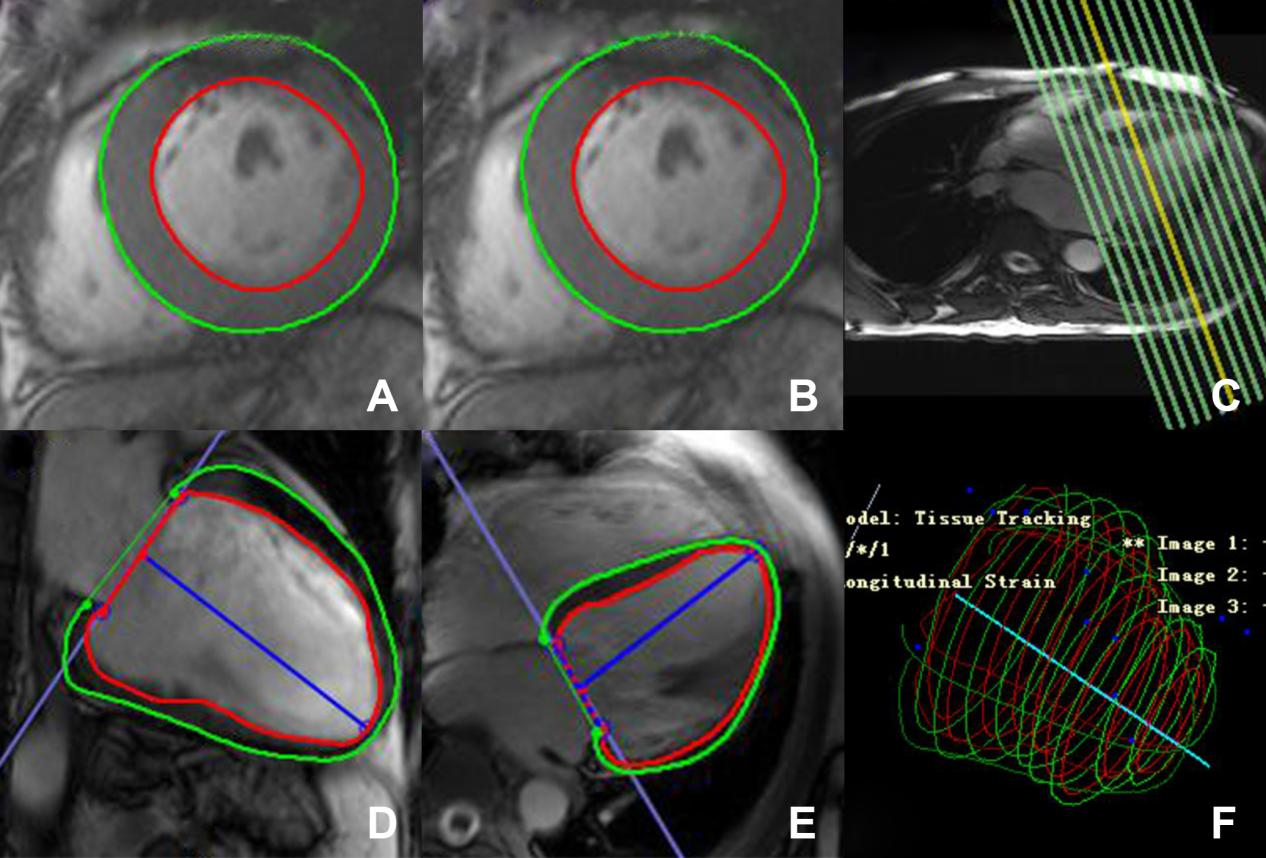
LV volume was calculated, and functional parameter image analysis was performed using commercial software (cvi42; Circle Cardiovascular Imaging, Inc., Calgary, AB, Canada) by two skilled radiologists with >3 years of CMR experience. The endo- and epi-cardial contours of the LV were contoured manually per slice on the end-diastole and end-systole images, and the papillary muscles and moderator bands were cautiously excluded. The LV volume and functional parameters, including end-diastolic volume, end-systolic volume (ESV), LV stroke volume (LVSV), LVEF, and LV mass were automatically calculated(Additional file 1).
Identification and classification of AR in patients with T2DM
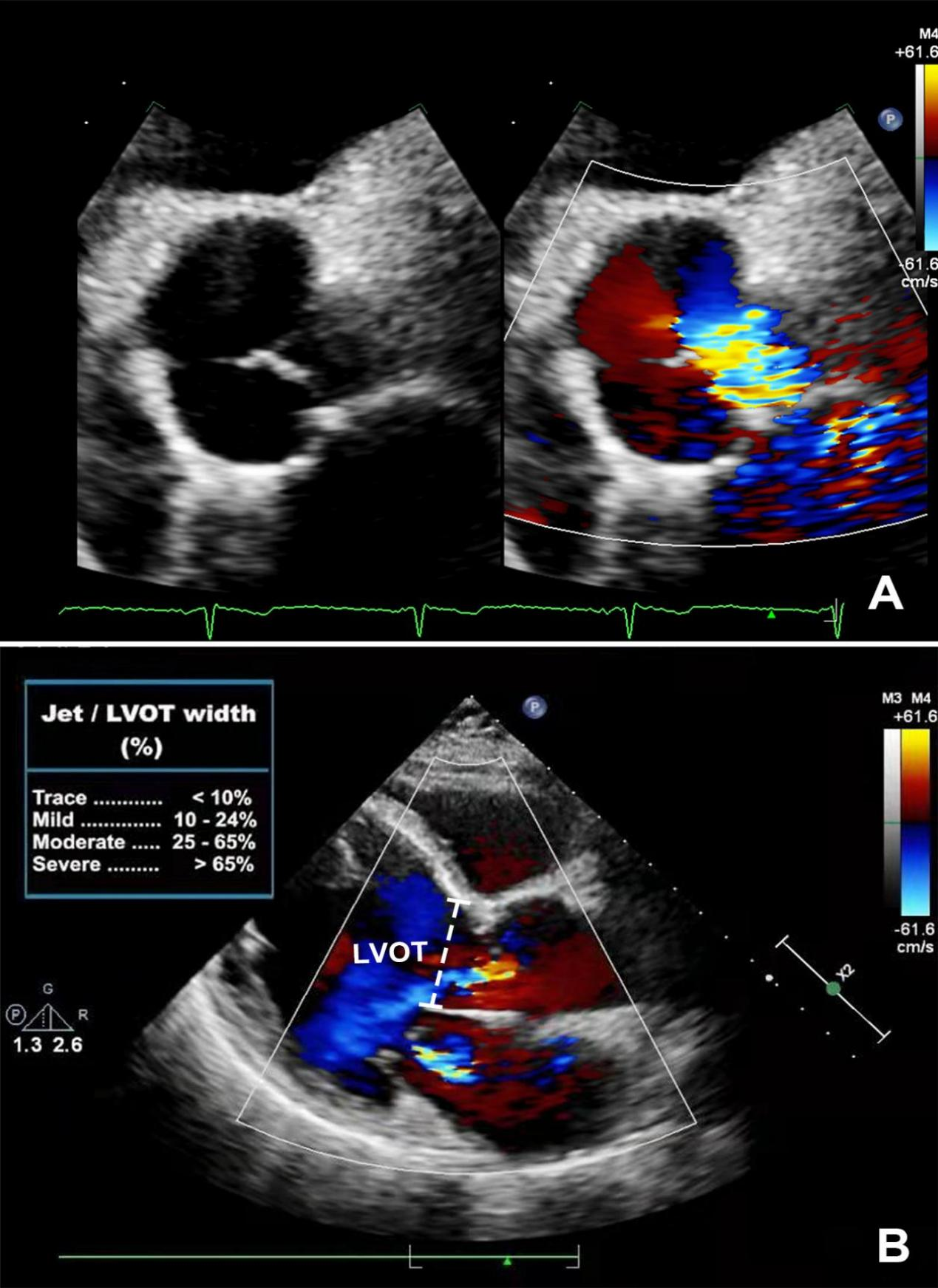
Echocardiography could facilitate the quantitative calculation of regurgitant volume and fraction, which can equally provide a better quantization of AR severity [13-15]. Color flow Doppler ultrasonography of the parasternal long-axis view provides an estimate of the regurgitant orifice size. The color jet diameter (or width) immediately below (within 1 cm) the aortic valve was measured in diastole. The jet diameter-to-left ventricular outflow tract (LVOT) diameter ratio was calculated as Jet/LVOT width (%). This ratio helps assess the degree of regurgitation: trace, <10%; mild, 10%–24%; moderate, 25%–65%; and severe, >65% [16, 17](Additional file 2).
LV strain analysis
Each voxel of the myocardium was pursued on the horizontal four-chamber long-axis, vertical two-chamber long-axis, and short-axis cine slices. The software automatically analyzed the global LV strain variables, including PS, peak systolic strain rate (PSSR), and peak diastolic strain rate (PDSR). Each strain parameter had three values in different directions (radial, circumferential, and longitudinal). The radial strain had a positive value due to myocardium thickening during LV contraction. The circumferential and longitudinal strains had negative values because the myocardium shortened during contraction [18, 19].
Reproducibility of LV strain
The intraobserver variability of LV global strain parameters was obtained by an experienced investigator by comparing the measurements in 80 randomly selected cases analyzed by the same observer after 1 month. The interobserver variability was evaluated by comparing the measurements from the same group by another independent double-blinded skilled observer.
Statistical analysis
Continuous data were assessed using the Shapiro-Wilk test and the Levene variance test to assess for distribution. Continuous variables, including low-density lipoprotein cholesterol level, eGFR, LVEF, and circumferential and radial PS were expressed as mean ± standard deviation. Moreover, the longitudinal PS among the three groups was compared via a single factor analysis of variance. The median (interquartile range: 25%–75%) was calculated for those with non-normal distribution. The Kruskal-Wallis H test was used for a multi-component comparison, and the Mann-Whitney U test was utilized to compare patients with T2DM who presented with AR and those without. Spearman’s correlation was applied to analyze the correlation between LV global PS (radial, circumferential, and longitudinal), regurgitation degree, duration of diabetes, and blood lipid levels. The absolute values of strains (circumferential and longitudinal) were used in the correlation analysis to eliminate confusion caused by the negative value. Variables with a P value of <0.1 and the absence of collinearity in the univariate analysis were included in the stepwise multiple linear regression model adjusted for sex, age, BMI, systolic blood pressure, and resting heart rate. Inter- and intra-observer variabilities were assessed using intraclass correlation coefficient (ICC). All analyses were performed using a two-tailed test, and a P value of <0.05 was considered statistically significant. All analyses were performed using the Statistical Package for the Social Sciences software (version 24.0; IBM, Armonk, New York, the USA) and GraphPad Prism (version 7.0a; GraphPad Software, San Diego, California, the USA).
{kind=link}
{kind=link}