Background: Tetralogy of Fallot (TOF) is one of the most common cyanotic congenital heart diseases. Pulmonary regurgitation is the most common and severe comorbidity after transannular patch (TAP) repair of TOF patients. It has not been confirmed whether a TAP repair with monocusp valve reconstruction would benefit TOF patients in perioperative period compared to those without monocusp valve reconstruction. The purpose of the study is to review and analyze all clinical studies that have compared perioperative outcomes of TOF patients undergoing TAP repair with or without monocusp valve reconstruction and conduct a preferable surgery.
Methods: Eligible studies were identified by searching the electronic databases. The primary outcome was perioperative mortality. Secondary outcomes included cardiopulmonary bypass time, aortic cross-clamp time, ventilation duration, ICU length of stay, hospital length of stay, and perioperative right ventricular outflow tract (RVOT) pressure gradient. The meta-analysis and forest plots were drawn using Review Manager 5.3. Statistically significant was considered when p-value ≤ 0.05.
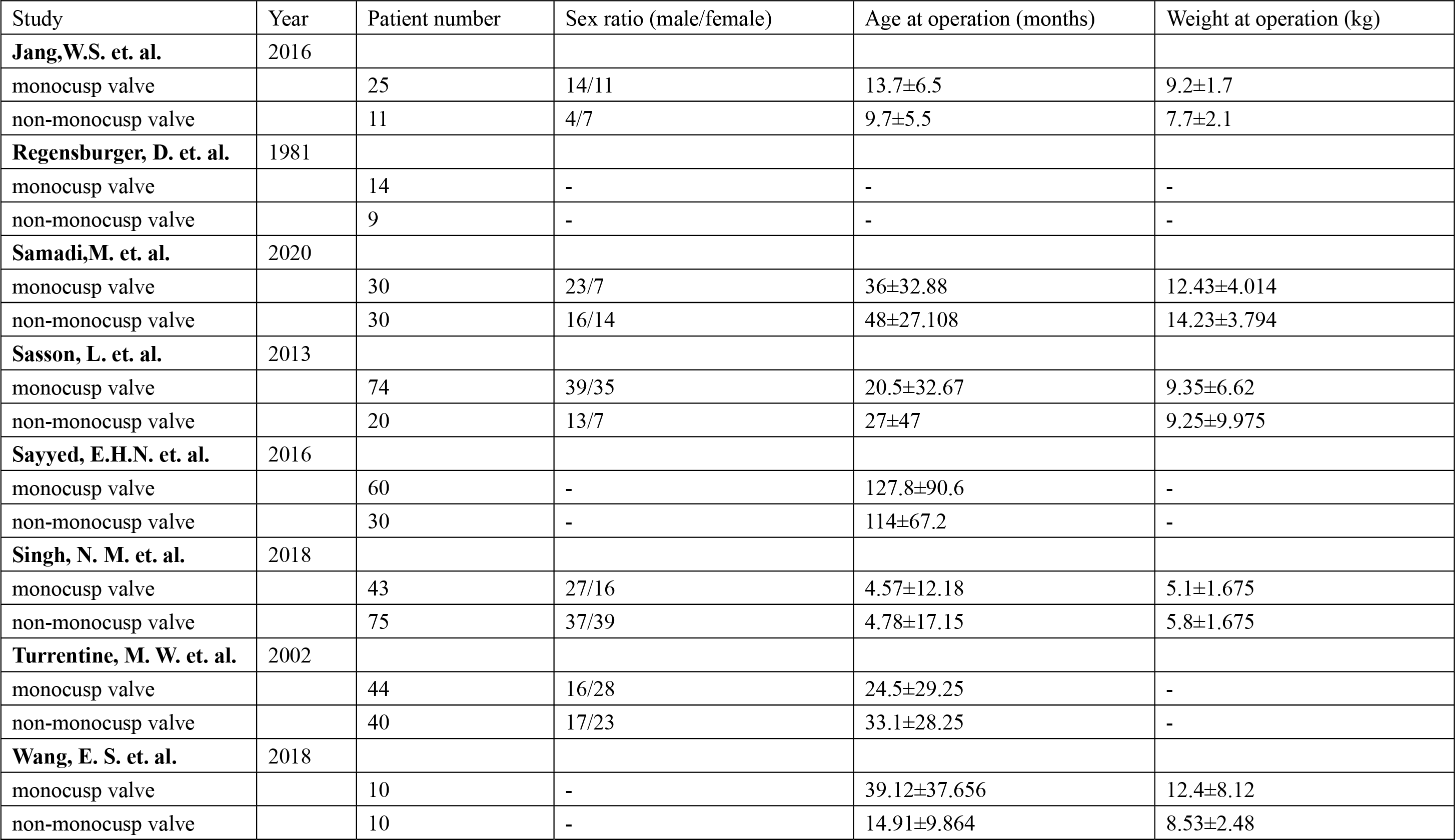
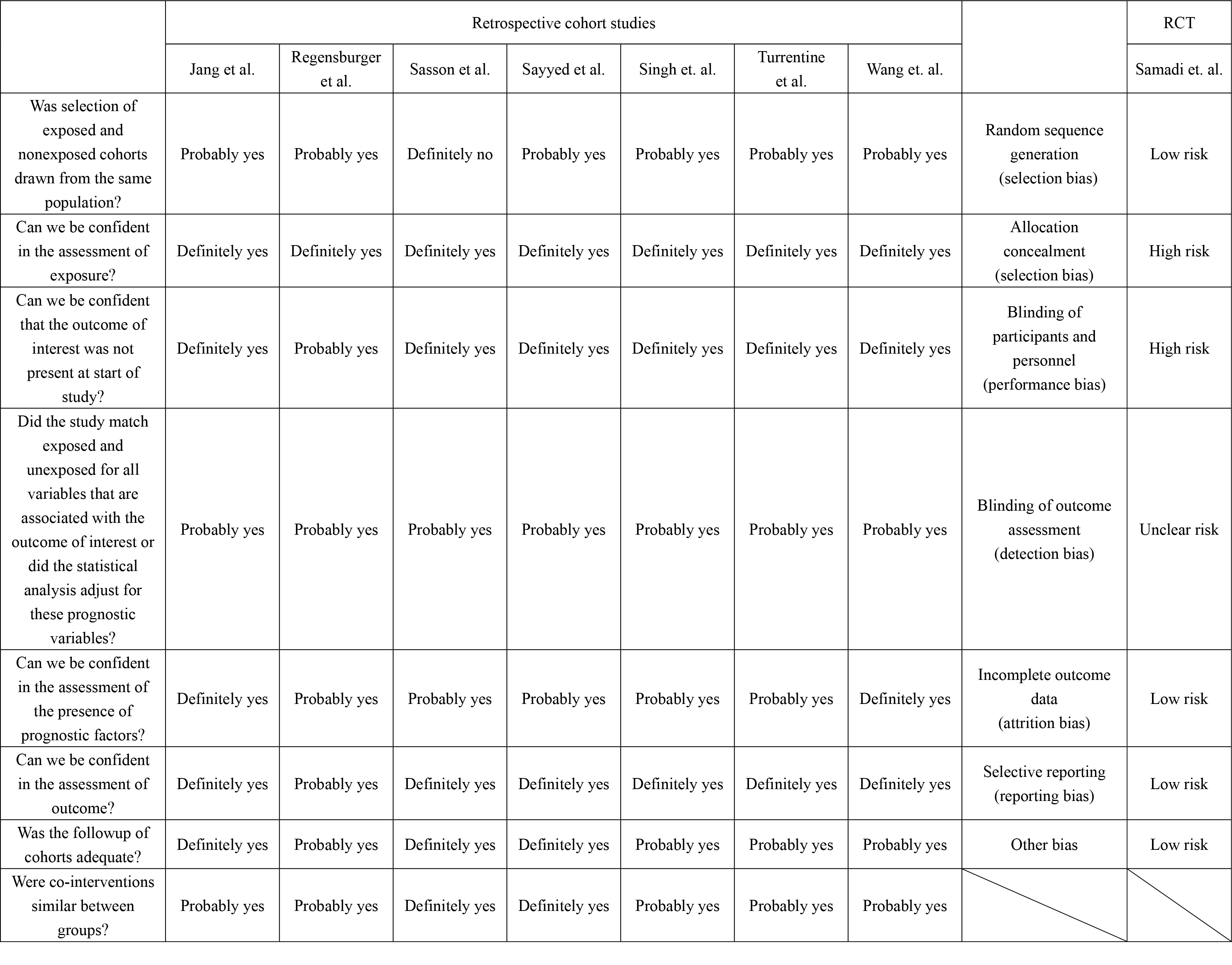
Results: Eight studies were included which consisted of 7 retrospective cohort study and 1 randomized controlled trial. The 8 studies formed a pool of 526 TOF patients in total, in which are 300 undergoing TAP repair with monocusp valve reconstruction (monocusp group) compared to 226 undergoing TAP repair without monocusp valve reconstruction (non-monocusp group). It demonstrated significant differences between two groups in perioperative cardiopulmonary bypass time (21.86, 95% CI 16.51-27.21), perioperative aortic cross-clamp time (11.20, 95% CI 1.06 - 21.34), mean length of ICU stay (-1.55, 95% CI -3.90 - -0.81), and the degree of perioperative PR (OR=0.02, 95% CI 0.00 - 0.15).
Conclusion: Transannular patch repair with monocusp valve reconstruction seems to have significant advantages on some perioperative outcomes of TOF patients. Large, multicenter, randomized, prospective studies focusing on differences between TAP repair with and without monocusp valve reconstruction are needed.
{kind=link}
{kind=link}