Study design and participants
This trial was a randomized, controlled, and open-label study. The main objective of the trial was to examine the effects of OLL1073R-1 yogurt on the incidence of influenza among women healthcare workers [15]. This paper details the secondary, psychological health-related outcomes monitored in the same trial.
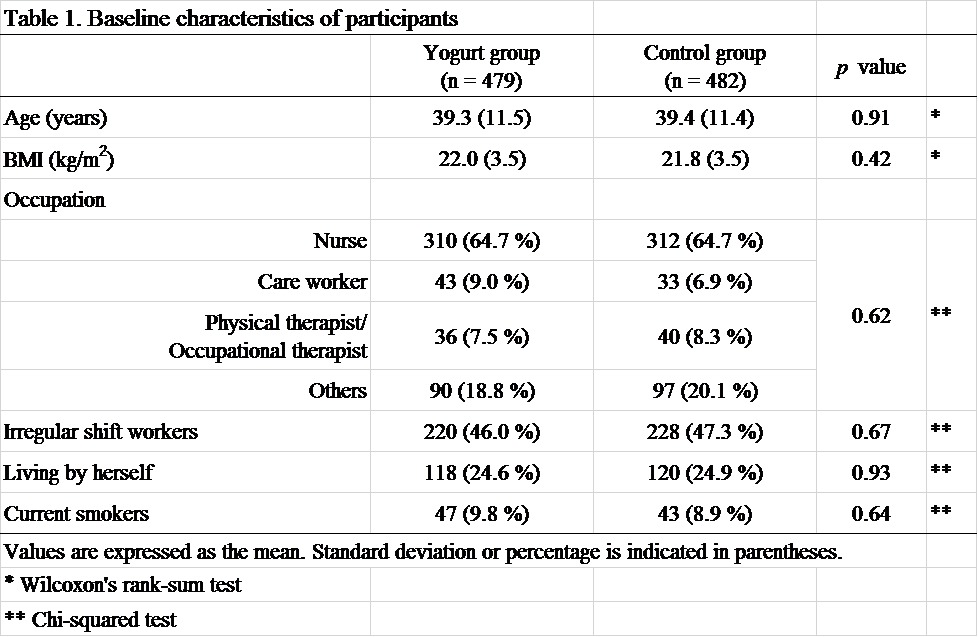
The main contents of methods of the present trial were explained in the previous report [15]. We estimated that a sample size of 600 participants in each group would be required to detect the effects of OLL1073R-1 yogurt on the incidence of influenza. Participants were recruited from 23 medical institutions in Ehime prefecture, Japan, from August to September, 2016. Women (aged ≥ 20 years) who were currently employed as medical or welfare-related professionals at medical institutions in Ehime prefecture and could understand the study purpose were selected, with written informed consent. The exclusion criteria were as follows: (1) pregnancy; (2) contracting influenza during the period from July 2016 to the date of providing written informed consent; (3) allergic responses to dairy products; (4) lactose intolerance; (5) instructed to restrict calorie intake by a physician; (6) history of diseases involving the immune system (e.g., rheumatism, cancer, thyroid disorder, systemic lupus erythematosus, myasthenia gravis, Graves’ disease, scleroderma); (7) participation in other clinical trials within the past 3 months; and (8) judged as unsuitable by the principal physician for other reasons. Of the 1,026 women who agreed to participate in this study, 20 infringed the exclusion criteria and 24 declined to participate after the agreement. Therefore, 982 women were examined at the screening session. By the day of the examination session, 20 women infringed the exclusion criteria and one declined participation. Consequently, 961 women (aged 20–71 years) were enrolled in the present study.
All participants were instructed not to consume any yogurt or fermented dairy foods from the day of agreement to that of random assignment. A total of 961 women were assigned to either the yogurt group (n = 479) or the control group (n = 482) through block randomization within three strata: institutions of employment, age, and having a plan of influenza vaccination or not.
Participants in the yogurt group consumed the test yogurt daily for 16 weeks (from November 14, 2016 to March 5, 2017), whereas those in the control group did not consume yogurt during this period. Furthermore, all participants were instructed not to consume any other yogurt or fermented dairy products throughout this trial. The participants answered self-administrated questionnaires at baseline and after 16 weeks. In addition, participants were provided with a “health notebook” to record changes in their lifestyles, intake of the test yogurt (for the yogurt group), and intake of any other yogurt or fermented dairy foods (for both groups) during the trial period. During the trial, four and 12 participants in the yogurt and control group declined participation, respectively. In the control group, two participants did not attend the examination session and one did not complete the self-administered questionnaires 16 weeks later. In addition, two and four participants in the yogurt group and control group, respectively, revealed that they were pregnant during the trial, thereby infringing the exclusion criteria. Figure 1 shows the sampling scheme throughout this study.
Test yogurt
The test food was “Meiji Probio Yogurt R-1” drink type (Meiji Co., Ltd., Tokyo, Japan), which is currently available on the market. This yogurt is manufactured using two lactic acid bacterial species, namely L. bulgaricus OLL1073R-1 and a strain of Streptococcus thermophilus, originally isolated from traditional Bulgarian yogurt. One bottle contains 112 mL of drinkable yogurt and provides 76 kcals, 13.9 g carbohydrate, 0.67 g fat, 3.6 g protein, and ≥ 1.12 × 109 CFU (colony forming units) of L. bulgaricus and S. thermophilus.
Outcome measurement
The participants completed the self-administrated questionnaires discussed below at baseline and after 16 weeks.
Quality of sleep
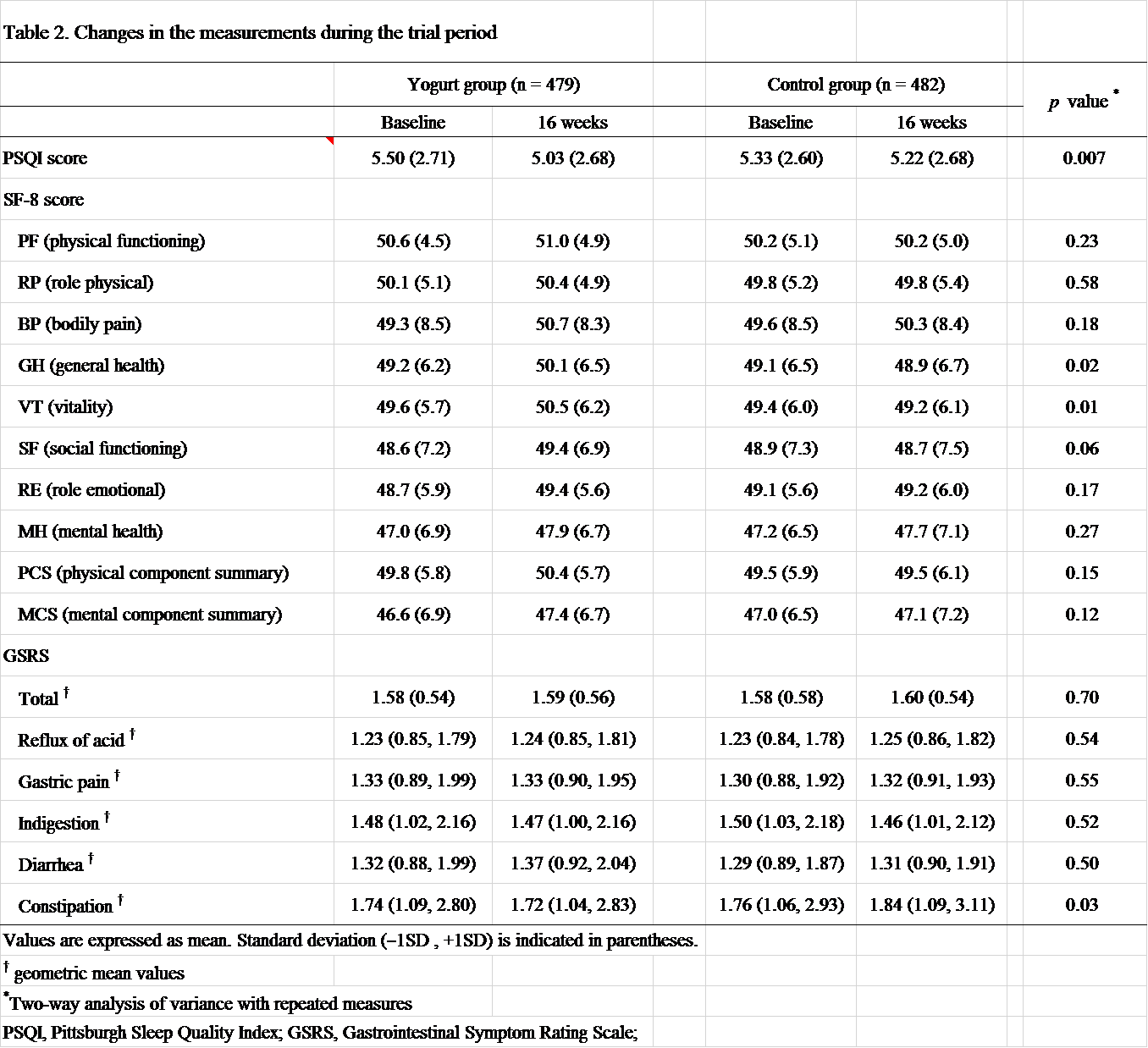
The Pittsburgh Sleep Quality Index (PSQI) was used as an index of subjective sleep condition [16], as it is established that dairy products exert beneficial effects on relaxation and quality of sleep [17]. The questionnaire is self-administered, and the participants were asked to answer the questions according to their quality of sleep (i.e., onset, duration, efficiency, difficulty, medication, and daytime sleepiness) during the previous 1 month. Each answer is converted into the score and the total score reflects the comprehensive sleep condition. Higher scores represent worse condition.
Subjective QOL
The eight-item Short Form Health Survey (SF-8) was used to evaluate subjective QOL [18]. The effect of OLL1073R-1 on improving mood status have been previously reported [13]. Therefore, we examined its role in improving psychiatric QOL. The SF-8 is a generic questionnaire widely used to compare the impact of different medical conditions, and as an outcome measure of different therapeutic interventions. The questionnaire is self-administered, and the participants were asked to complete eight questions according to their experiences during the previous 1 month. The questions were divided into eight subscales and two dimensions that described the overall health status. The eight subscales were physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). The two dimensions are physical component summary (PCS) and mental component summary (MCS), were calculated based on the scores of the eight subscales using specific standardized algorithms. The scores of each scale ranged from 0 to 100, with high scores representing better QOL.
Gastrointestinal condition
The Gastrointestinal Symptom Rating Scale (GSRS) was used as an index of gastrointestinal condition [19, 20], as it is established that probiotics improve gastrointestinal symptoms, such as constipation [2]. The GSRS consists of 15 questions; the participants answered all questions according to their gastrointestinal condition during the previous 1 week. We evaluated the total score and five subscale scores (i.e., reflux of acid, gastric pain, indigestion, diarrhea, and constipation). The scores of the total and each subscale ranged from 1 to 7, with higher scores representing worse condition.
Statistical analysis
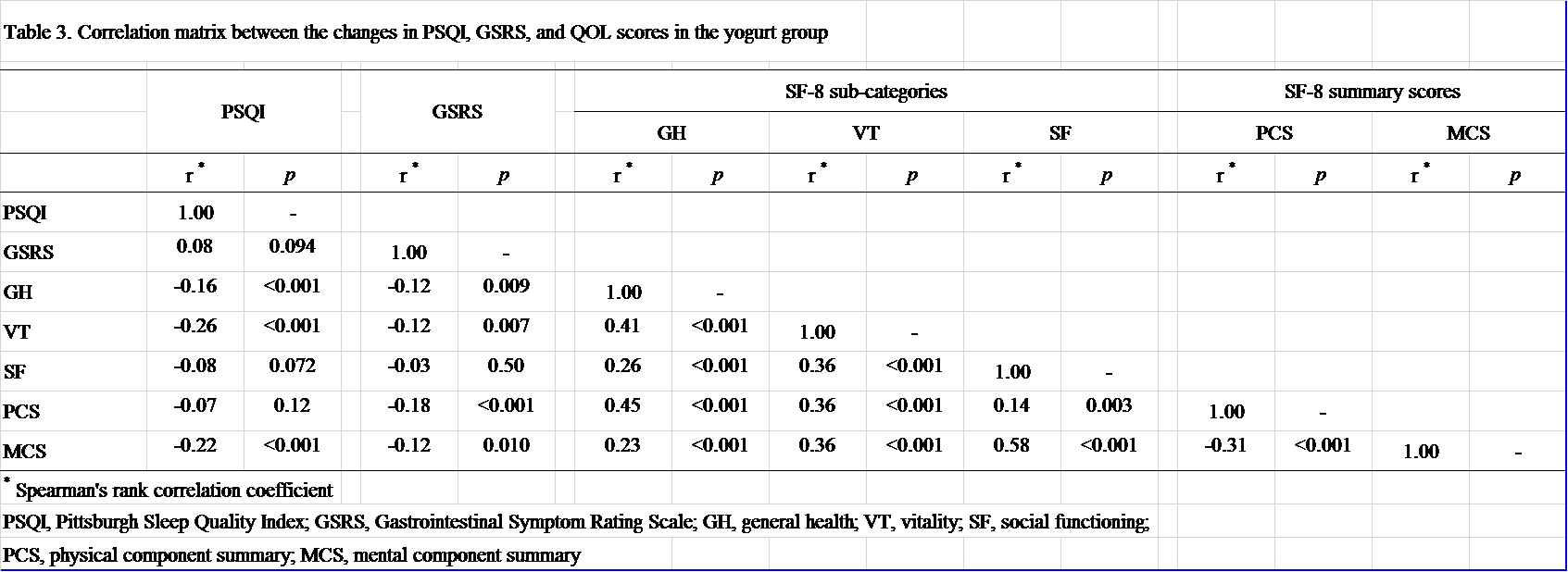
All statistical analyses were performed using based on intention-to-treat analysis in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Differences in the means of the indices between the two groups at baseline and after 16 weeks were analyzed using an unpaired t-test. The effects of the intervention on the scores of the PSQI, SF-8, and GSRS were analyzed through two-way analysis of variance with repeated measures. Owing to the non-normal distribution of the GSRS score, geometric means were calculated and used for analysis. In case of participant withdrawal from the study, the values for PSQI, SF-8, and GSRS obtained at baseline were used as those after 16 weeks. In the yogurt group, the correlation between the changes in QOL scores and changes in PSQI and GSRS scores were analyzed using Spearman’s rank correlation analysis. For the incidence of adverse events in both groups, the rates were analyzed in 10 categories using the chi-squared test. In all analyses, p < 0.05 (two-sided) denoted statistical significance.
{kind=link}
{kind=link}
{kind=link}