Among all cancers, Liver hepatocellular carcinoma is the fifth most frequently diagnosed cancer, ranking as the third leading cause of cancer-related death, seriously impacting human health [28]. Currently, the main LIHC treatment strategies include surgical resection, microwave ablation, radiofrequency ablation and transcatheter arterial chemoembolization (TACE) [29, 30]. Although surgical resection is believed to have a definitive curative effect for LIHC, the clinical outcome is still poor due to frequent recurrence and metastasis [31–33]. Additionally, most LIHC cases are detected in advanced stages with the invasion of major blood vessels, obvious extrahepatic metastases or poor liver function, making them unfit for surgical resection [34]. Better biomarkers for predictive and prognostic molecules for LIHC are still required.
In this study, bioinformatics and comprehensive analyses of multiple datasets were used to screen genes that proved to be novel prognosis factors for LIHC. Firstly, we compared the translational profiles between normal and cancerous samples to obtain DEGs. GO and KEGG enrichment analysis was performed to interpret the functions and pathways of DEGs. The enriched BPs included eukocyte migration, organelle fission, nuclear division, chromosome segregation, humoral immune response, and so on. These processes had strong relationship with LIHC progression. The processes of GO CCs and GO MFs are also typically representative features of LIHC progression. The enriched KEGG pathways included neuroactive ligand-receptor interaction, cytokine-cytokine receptor interaction, cell cycle, and so on, which are also associated with LIHC. Then, co-expression network analysis by WGCNA identified that blue module was significantly associated with LIHC traits. The genes in these modules were taken intersection with DEGs between pathology stages I and IV. Finally, CDC20, CDCA5, CDCA8, KIF2C and KIFC1 were screened out. Using GEPIA based on the TCGA database, we proved the expression levels of CDC20, CDCA5, CDCA8, KIF2C and KIFC1 were significantly up-regulated in LIHC. And the survival analysis showed that high expression of these genes was associated with poor prognosis. Moreover, univariate cox analysis showed that the high expression of CDC20, CDCA5, CDCA8, KIF2C and KIFC1 would make a poor prognosis. Further multivariate cox proportional hazard regression analysis revealed that high CDCA8 expression was related to inferior prognosis, which indicated that CDCA8 could serve as an independent risk factor to predict the prognosis of LIHC.
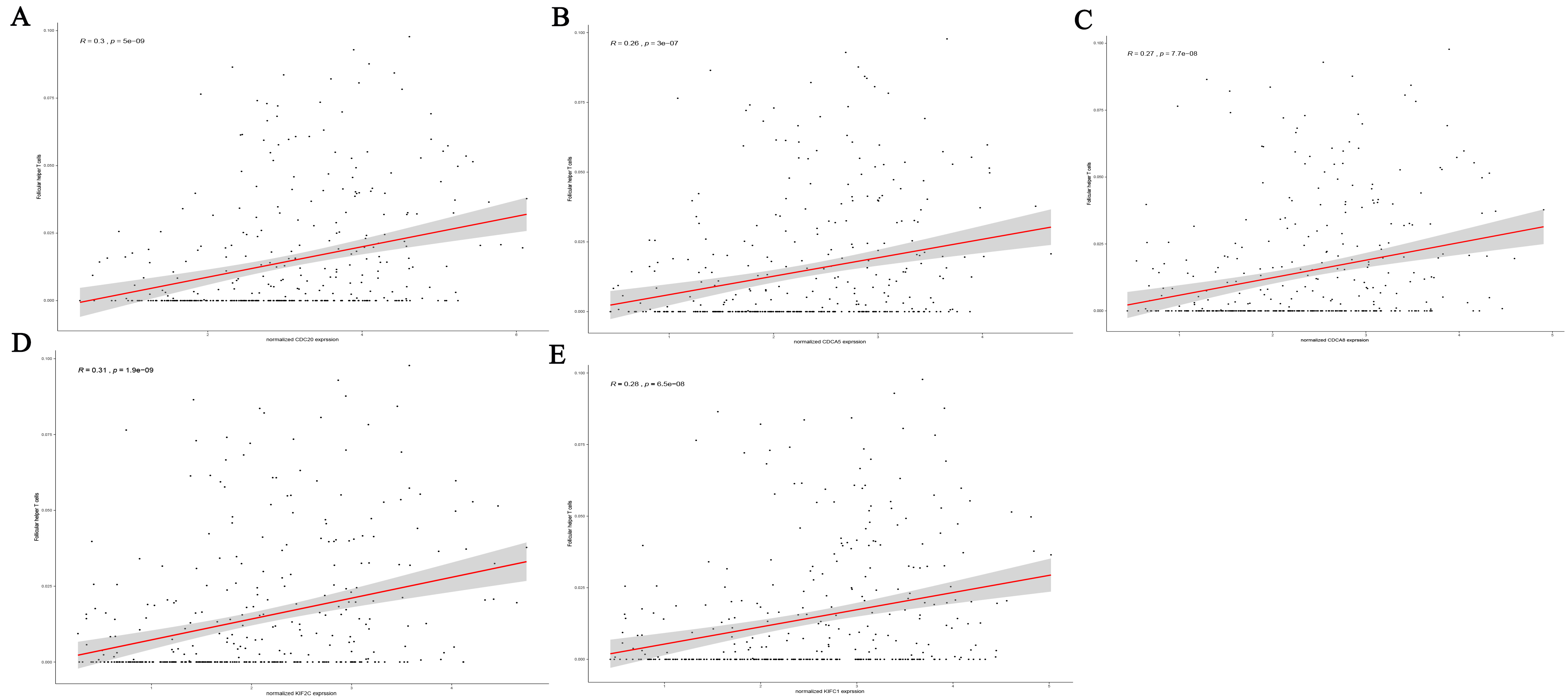
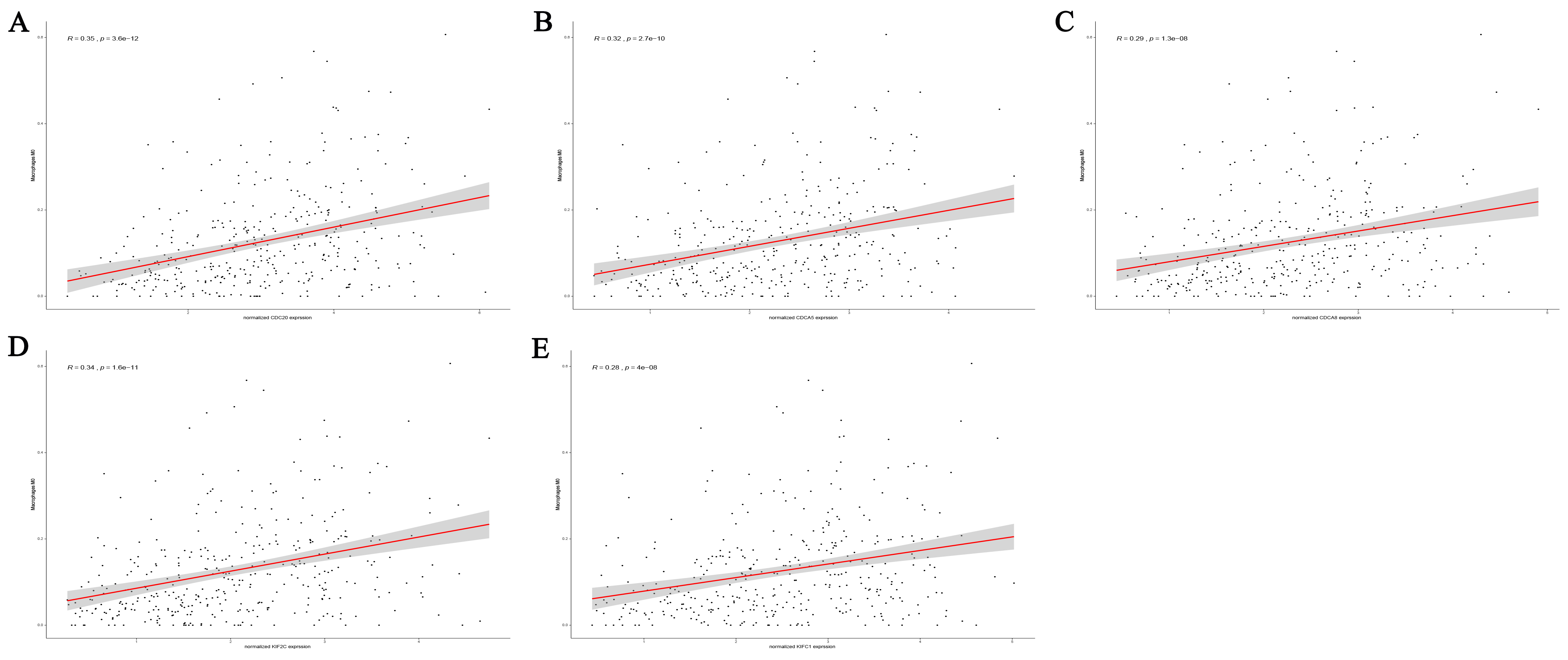
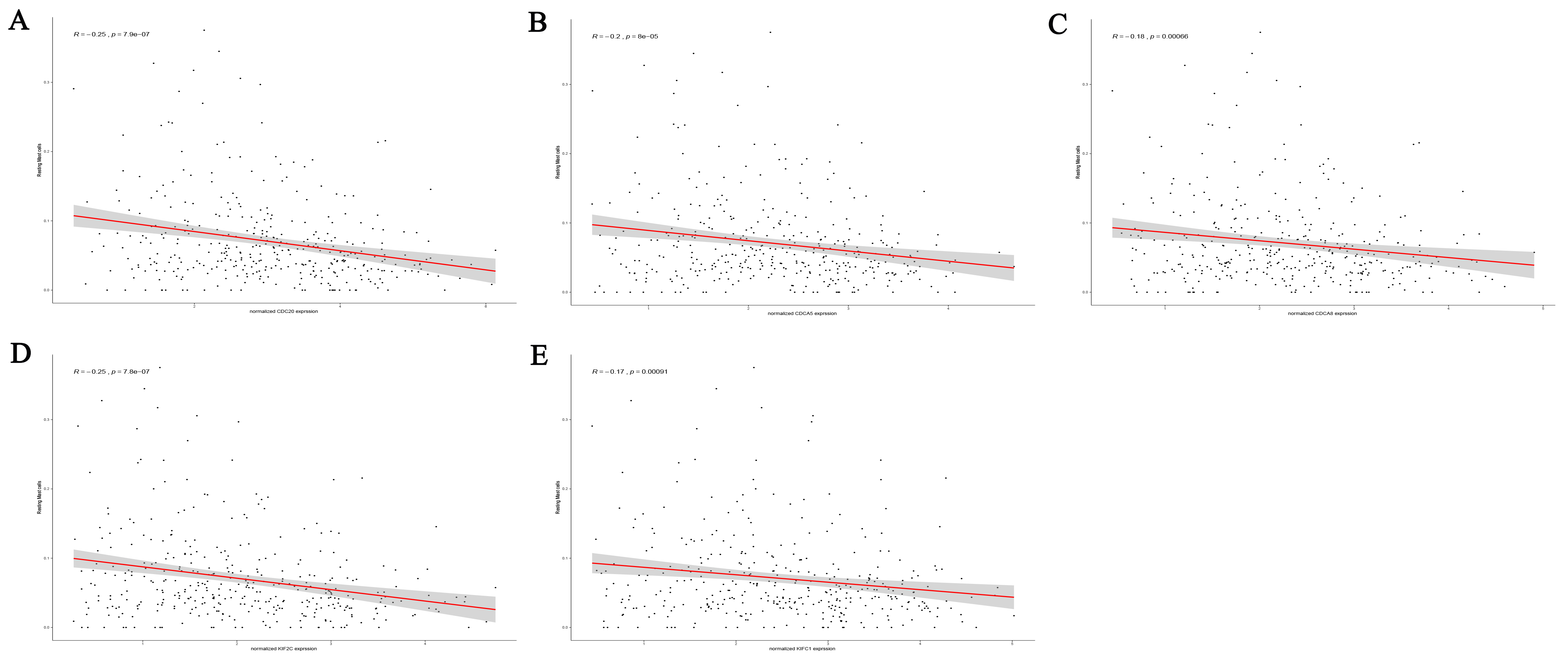
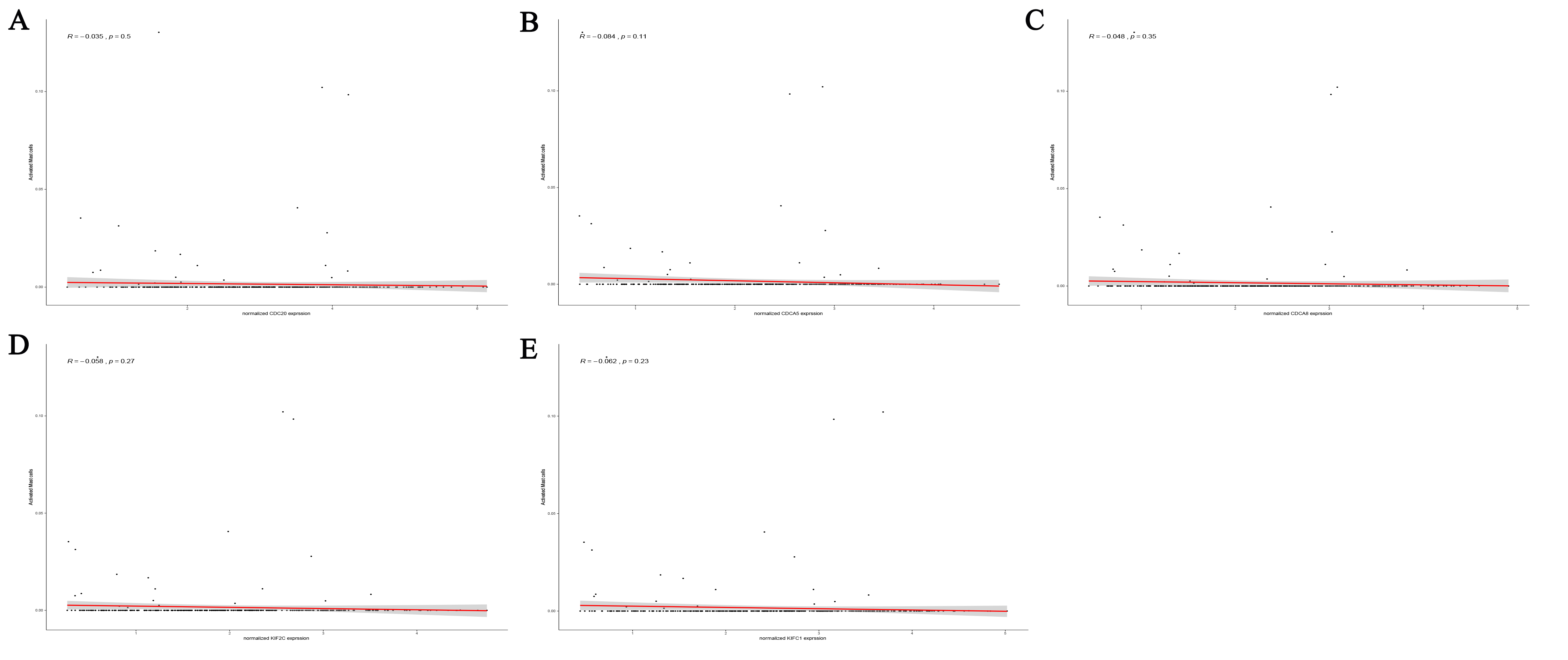
Strikingly, the 5 genes have been reported correlated with clinical outcomes of a huge number of solid tumors. Cell division cycle 20 homologue (CDC20), also called Fizzy, specifically activating the anaphase-promoting complex-cyclosome, promoting ubiquitination and proteolysis of cell-cycle-regulatory proteins, which is essential for anaphase-promoting complex activity, initiation of anaphase, and cyclin proteolysis during mitosis [35]. In recent years, mounting evidence has revealed that CDC20 plays an oncogenic role in human tumorigenesis. Overexpression of CDC20 was observed in a variety of human tumors, including pancreatic cancer [36], breast cancer [37], prostate cancer [38], lung cancer [39], colorectal cancer [40] and liver hepatocellular carcinoma [41]. Li et al. reported that overexpression of CDC20 was observed in 68% liver hepatocellular carcinoma tissues compared to adjacent non-tumor liver tissues. Moreover, high levels of CDC20 were positively correlated with gender, tumor differentiation, and TNM stage [41]. In our study, we found the overexpression of CDC20 may result in an unfavorable prognosis and promote TEM immune infiltration in LIHC patients. Cell division cycle associated 5 (CDCA5), is an important element for the interaction between cohesin and chromatin in interphase. As reported, the expression of CDCA5 was upregulated in LIHC tissues compared to paracancerous tissues and had a negative correlation with patient survival. Further study showed that CDCA5 promotes oncogenesis by enhancing cell proliferation and inhibiting apoptosis via the AKT pathway in liver hepatocellular carcinoma, plays an important role in LIHC progression [42]. These results were consistent with our findings. The cell division cycle associated 8 (CDCA8) plays an important role in mitosis [43]. CDCA8 is a putative oncogene that is up-regulated in many types of cancer tissues, such as lung cancer [44] and gastric cancer [45]. While, little is known about its role in liver hepatocellular carcinoma. Our study revealed that CDCA8 was significantly upregulated in LIHC and linked to poor prognosis. Besides, CDCA8 plays a vital role in regulating immune cell of TEM and could serve as an independent risk factor to predict the prognosis of LIHC. Kinesin family member 2C (KIF2C), the kinesin-like protein functioning as a microtubule‐dependent molecular motor, participates in spindle assembly and microtubule disaggregation, thereby determinately regulating cell cycle during mitosis [46–49]. A recent study firstly demonstrated KIF2C was substantially higher expression in tumor tissues than adjacent nontumor tissues, upregulated PCNA and CDC20 expression and was significantly involved in growth promoting pathways, fully confirming our results that it could serve as a prognostic indicator and confer a novel target for clinical treatment. Kinesin family member C1 (KIFC1), also known as HSET, is a minus end-directed motor protein [50], which is a critical role in centrosome clustering in cancer cells [51]. Fu x et al. investigated the expression of KIFC1 in paired liver hepatocellular carcinoma tissues and adjacent non-cancerous tissues and found that the expression of KIF2C was upregulated and connected with a poor prognosis of LIHC [52]. Our analyses further revealed that the overexpression of KIFC1 was a novel predictive marker in patients with LIHC and involved the regulation of immune cell in LIHC TEM.
The association of inflammation and cancer was firstly hypothesized by Rudolf Virchow observations in 1863 as chronic irritation theory. Virchow found that certain cancers are associated with inflammatory macrophages [53]. In recent years, more and more studies have proved the important role inflammatory cells played in the development of cancer. Neutrophils, monocytes, lymphocytes, dendritic cells, eosinophils and mast cells are the commonly observed cells in tumor stroma although their count depends on cancer type [53, 54]. In this study, we illustrated the percentage distribution of immune cells in LIHC TEM, finding macrophages M0, macrophages M1, macrophages M2, resting memory CD4 + T cell and CD8 + T cells accounted for most of the immune cells. Remarkably, increasing number of studies showed that macrophages facilitate cell proliferation, angiogenesis, metastasis and invasion, which were important in the initiation, development and metastasis of primary hepatocarcinoma [55].In the early stage of tumorigenesis, M1 macrophages eliminate the tumor cells as soldiers of adaptive immunity. However, in advanced stages, M1 macrophages replaced with M2-type. M2 macrophages suppress the adaptive immune system and promote the cancer proliferation, angiogenesis and extracellular matrix remodeling as well. Eventually, tumor cells escape from the immune barriers and invade [56, 57]. Additionally, CD4 + T cells and CD8 + T cells were confirmed to participate in immune recognition and escape of LIHC [58]. Actually, tumour infiltrating lymphocytes (TILs) form a large component in solid tumours, in an attempt by the host to mediate an antitumour reaction [59]. However, this cellular response can be dysfunctional with a higher proportion of CD4+ (helper or T regulatory cells) to CD8 + cells. This promotes immune tolerance and has been shown to confer a worse prognosis [60]. E.A. Said et al found that the binding of PD-L1 (expressed on other cells) to its receptor PD-1 on macrophages promotes IL-10 release and thereby CD4 + T cell repression [61]. Effector CD8 + cells within LIHC tumors show intense PD-1 expression and the number of PD-1 + CD8 + cells was found to be related to disease progression and post-operative recurrence [62]. Since the existing treatment strategies for LIHC have great limitations, immunotherapy is a promising therapeutic option. Our results revealed the 5 novel biomarkers expression levels had a crucial association with parts of immune cells, which suggested these genes may involve in the level regulation of the immune cells of TEM in LIHC, may help to promote the application of immunotherapy in liver cancer.
{kind=link}
{kind=link}
{kind=link}
{kind=link}