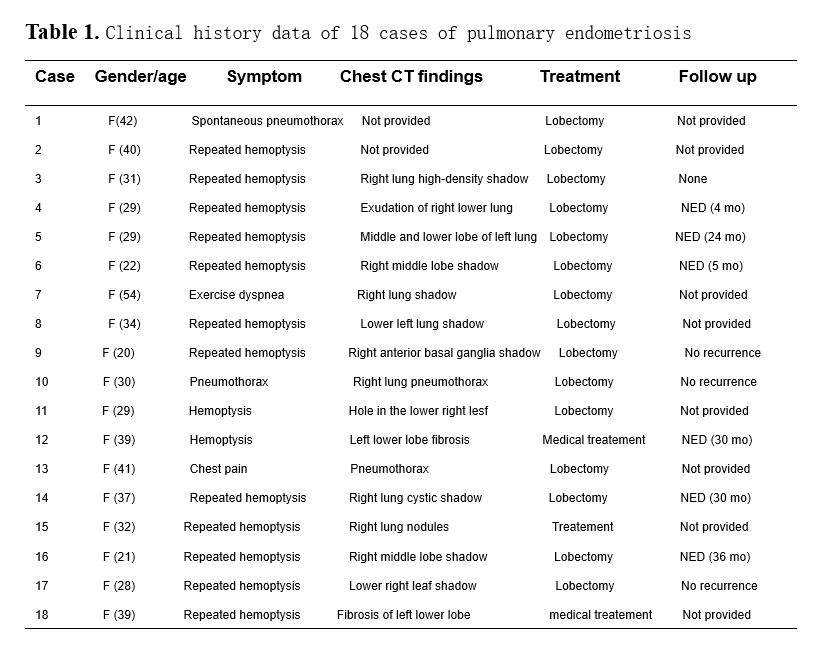
We analyzed this case as well as 18 other reported cases of lung endometriosis (presented in Table 1). The age of onset was between 19 to 54 years. Patients often sought out doctors due to repeated menstrual hemoptysis, and most patients had a history of miscarriage or uterine cavity surgery. The appearance of hemoptysis was consistent with the occurrence of the menstrual period. After menstruation, the hemoptysis subsided; consistent with this, most patients exhibited imaging changes during the menstrual period, but the imaging findings disappeared after the menstrual period. Almost all patients reported on underwent local lobectomy, and histopathology confirmed the presence of endometrial glands, interstitial cells, hemosiderin deposits, fibrous tissue hyperplasia, or similar pathological findings in the lung tissue. Some patients underwent additional immunohistochemical detection of ER, PR, CD10, or CD68, for instance, and the results suggested the presence of endometrial tissue. In all patients, hemoptysis, pneumothorax and imaging changes disappeared postoperatively, and no recurrence was reported.
Endometriosis is characterized by the growth of the endometrium outside the uterine cavity. It is a common gynecological disease that affects the fertility of women of childbearing age, with an incidence of approximately 15% in women of childbearing age [4]. It is generally considered to be a hormone-dependent disease [3]. Endometriosis mostly occurs in the pelvic cavity, while it can also occur outside the pelvic cavity. A rare form of endometriosis outside the pelvic cavity is lung endometriosis, which accounts for about 20% of pleural endometriosis [1, 2]. As early as 1938, Schwarz described pulmonary endometriosis for the first time [5]. However, it is an extremely rare disease with complex etiology and unclear pathogenesis, and as its clinical and imaging findings are not specific, it can easily be misdiagnosed.
At present, several clinical features of lung endometriosis have been reported, including repeated hemoptysis, coughing, pneumothorax, hemothorax, and pulmonary nodules consistent with menstrual periods, but not all clinical features will appear at the same time. Among the above-mentioned clinical features, approximately 82% of lung endometriosis patients experience menstrual hemoptysis as their main symptom [6], while the remaining patients may present with menstrual pneumothorax, menstrual hemothorax, or other symptoms. X-ray or CT scans can assist in the diagnosis of lung endometriosis, although it can easily be misdiagnosed due to its non-specific symptoms and rare occurrence. Therefore, other diseases must be ruled out before a clear diagnosis can be made [7]. In our case, the young woman lived in an area with a high incidence of tuberculosis and had symptoms of hemoptysis, but did not have symptoms such as low-grade fever and night sweats. CT showed no nodules, and the sputum smear test for Mycobacterium tuberculosis was negative, therefore tuberculosis was excluded.
The typical pathological features of endometriosis are endometrial glands, interstitium and hemosiderin deposition under the microscope [8]. However, compared with pelvic endometriosis, these microscopic features might not all be seen concurrently in lung endometriosis. Ghigna et al. [9] reported that these three characteristics appeared at the same time only in 44% cases of lung endometriosis, while in the remaining cases only endometrial stroma was found. When only a small amount of endometrial stromal is found in lung tissue, the diagnosis is rendered more difficult [10]. In addition, it is sometimes difficult to distinguish endometrial stroma and inflammatory cells by H&E staining. Therefore, immunohistochemical detection is needed to assist in the diagnosis of lung endometriosis [11]. In the case we report here, ectopic endometrium in the lung tissue led to alveolar hemorrhage, hemosiderin deposition, chronic inflammation and fibrosis due to long-term incomplete absorption or excretion. Only few glandular epithelial cells were seen in the alveolar cavity and vascular cavity, and CK markers were positive, while ER, PR, and CD10 were negative. Prussian blue staining for hemosiderin was positive. Combining the above histopathological and immunohistochemical findings with the history of miscarriage, clinical symptoms, imaging changes and the exclusion of other lung diseases, the diagnosis of lung endometriosis was made.
The pathogenesis of endometriosis is still unclear, but 8 theories exist:
-
Endometrial implant theory: This is the most common view. Sampson proposed that when the menstrual blood flows backward, the shed endometrium can enter the pelvic cavity through the fallopian tube and implants outside the endometrium [12, 13]. Local injuries such as the cervix, vagina, and vulva can therefore easily cause endometriosis [14, 15];
-
Body cavity epithelial metaplasia theory: Meyer et al. proposed that body cavity epithelium has the potential to differentiate into endometrial tissue [16]. It may be transformed into endometrial-like tissue by certain stimulations;
-
Iatrogenic endometrium implantation: This theory suggests a type of artificial endometrial transplantation to certain parts, such as to the abdominal wall scar after cesarean section or perineal side incision after childbirth. A history of multiple uterine cavity operations, repeated abortions, tubal drainage or similar, may therefore lead to endometriosis [16, 17];
-
Embryo theory: In the embryo, the accessory mesonephros, ovary germinal epithelium, pelvic peritoneum, rectovaginal septum, umbilical region, and other tissues evolve from body cavity epithelium, and they are able to differentiate into endometrioid tissue when stimulated by inflammation, which is more common on the surface of the ovary;
-
Induction theory: Under the induction of endogenous biochemical substances, undifferentiated peritoneal tissue can be transformed into endometrial tissue;
-
Genetic factors: Endometriosis has a certain genetic predisposition and family aggregation, and people with a family history are more likely to suffer from this disease;
-
Immune factors: There are reports and studies that speculate that diseased stem cells play an important role in the blood spread of epithelium and long-distance implantation [18, 19].
At present, there is no comprehensive treatment guideline for lung endometriosis. It is generally believed that treatment includes conservative drug treatment and surgical treatment. The most appropriate treatment method is selected based on the patient’s clinical symptoms, severity and requirements. The first choice for conservative treatment is Gonadotrophin releasing hormone agonist, which is now widely accepted. This treatment inhibits the release of estrogen and progesterone from the ovaries and results in a decrease in the level of estradiol in the plasma, mimicking a state of pseudomenopause in order to control the growth of lesions. However, gonadotrophin releasing hormone antagonist treatment is costly, can elicit many adverse reactions, needs to be carried out long-term, and is symptomatic rather than a cure [1]. In addition, the recurrence rate is high, and long-time treatment may also harm the patients’ ovulation and fertility [20]. Hence, most patients choose surgical treatment, especially pulmonary wedge resection. Compared with drug therapy, the recurrence rate is lower and the prognosis is better.
{kind=link}