3.1 No correlation between asthma and six criteria air pollutants
In this study, children’s asthma hospitalization peaked in late spring (from March to May) and fall (from September to November), as shown in Fig. 1. Bronchial asthma attack often occurs in the spring and fall [17]. The arrival of spring brings pollen allergy from grasses, weeds, and trees, and the fall means the transition to the cold days, which are common triggers of asthma attacks. There was a gender difference in childhood asthma (STable 1). Male children were significantly more likely to be sensitized to allergens [17]. Figure 2 showed that there was no significant association between the six common air pollutants, except for lag0 of SO2, lag3 of NO2, lag3 of O3 and lag0 of PM10. Subgroup analysis by gender and age showed no significant effects. The comparison of the trend pattern between the month average concentrations of six-air pollutant and asthma hospitalization was shown in Sfig.1. Except for O3, the peaks of SO2, NO2, CO, PM2.5, and PM10 concentrations were ahead of that of asthma hospitalization. Although it is not statistically significant, it still indicated that after the peak of O3 concentration, there was an increase in asthma-related hospital admissions. The monthly average relative humidity, temperature and average wind speed also matched with the hospital admissions, as shown in Sfig.2; however there was still no significant correlation .
3.2 1-OHPyr Levels In Urine Samples
In this study, the characteristics of the subjects being sampled were described in Table 1. All the asthmatic children adminstrated control medicine, such as inhaled corticosteroid (ICS), long-acting beta agonists (LABAs), short-acting beta agonists (SABAs), oral anti-allergic medicine, and immunomodulator. asthmatic and control subjects had healthy diets with fried or grilled food intake at 0–1 time/week, were living in the city, lived within 2 kilometers from schools, walked or were sent by electric bike to school, lived in homes with vent-out kitchens, and had non-smoking parents. The urinary 1-OHPyr level ranged from non-detected (ND) to 2.477 ng/ml in the asthma group and from ND to 0.156 ng/ml in the control group. The creatinine correction average value was 0.219 ± 0.33 µmol/mol in asthmatic children and 0.137 ± 0.052 µmol/mol. The geometric means of two groups were not significantly different. The coefficient of variation (COV) of 1-OHPyr concentrations in the asthma group was 150.5% (standard Deviation: 0.330, mean: 0.219), and was 38.4% (0.052, 0.137) in the control group. There were individual differences with the exposure levels of PAHs in the asthma group. In addition, the geometric mean of 1- OHPyr levels in the National Health and Nutrition Examination Survey (NHANES) 2003–2004 subsample 6–11 year old children was 119(in ng/g of creatinine), that was 0.05 µmol/mol Cr [18]. Compared with American children 1-OHPyr exposure level, the exposure level of 1-OHPyr of children in Nanjing was much higher.
Table 1
The characteristics of the subjects in this study
| Variable | Asthma group(history of allergy) | Control group | |
| male | 13(7) | 13 | |
| female | 7(3) | 7 | |
| Age (yrs) | 6.45 ± 2.3 | 7.23 ± 1.5 | |
| Medication (%) | | | |
| ICS/LABA | 100 | - | |
| SABA | 15 | - | |
| Singulair | 10 | - | |
| Anti-allergy medicine | 20 | - | |
| Immunomodulator | 50 | - | |
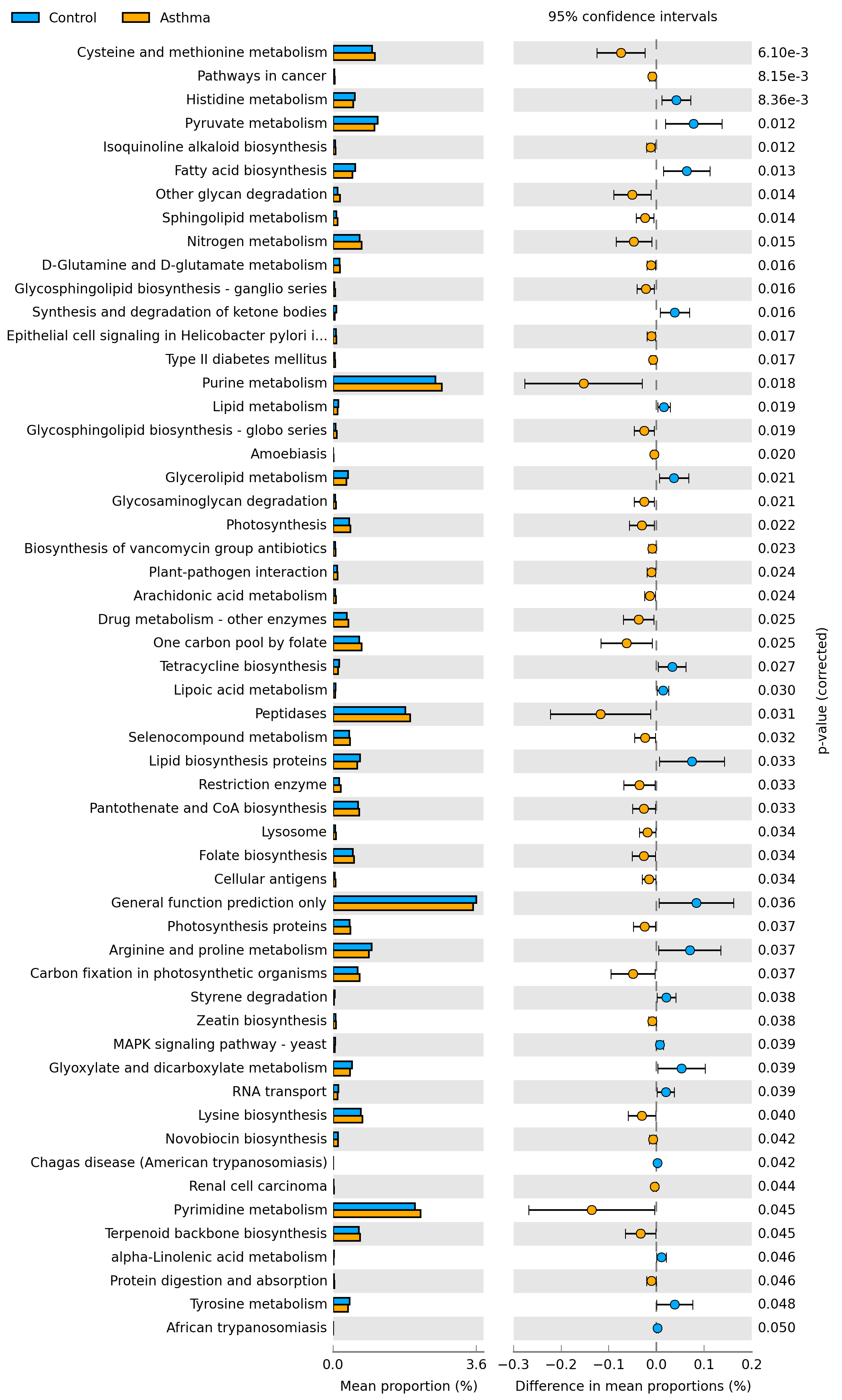
3.3 1-OHPyr was associated with children's commensal microbiota in the throat
After sequencing, a total of 2417101 sequences were produced after optimization, and 681 OTUs were obtained based on the 97% threshold. After classified and alignment with Silva database, the OTU table contained taxonomic information with 23 phylum levels and 346 species levels. Pan analysis, rank-abundance curve, and sob index were used to study the diversity of microbial communities in children with asthmatic or healthy children. The results in Sfig.3 showed that the microbial diversity and richness of the control group was more abundant than that of the asthmatic group. Rarefaction curve almost tended to approach an asymptote that reflected a perfect estimate of sampling.
The compositions of the two groups had remarkable similarity. The taxonomic composition of the microbial communities at the phylum level in asthmatic group and the control was shown in Fig. 3A and B, which mainly consisted of Firmicutes, Bacteroidetes, Proteobacteria, Actinobacteria, Fusobacteria and so on, and at genus level, mainly consisted of Streptococcus, Veillonella, Prevotella, Neisseria, Haemophilus, Actinomyce, Leptotrichia and so on (Fig. 3C and D). The significant differences in microbial communities were performed using the Wilcoxon rank-sum test. At the phylum level, the abundance of Proteobacteria was decreased (P = 0.0461) in the asthmatic group, and that of Firmicutes (P > 0.05) and Bacteroidetes (P = 0.0238) was increased. At the genus level, the abundance of Veillonella (P = 0.0159) and Prevotella(P = 0.0066) was increased (Fig. 4), and that of Neisseria and Haemophilus was decreased(P > 0.05) in asthma group. Multiple biological pathway, such as cancer, environmental adaptation, nucleotide metabolism and lipid metabolism were predicted from the throat metagenome by PICRUSt(Figure 5), and the detailed pathway was illustrated in Sig.4. Pearson correlation coefficient was applied to investigate the association between 1-OHPyr and microbiota diversity. There was some positive correlation between microorganism and 1-OHPyr level. Stomatobaculum༈r = 0.80, P < 0.0001༉, Selenomonas ༈r = 0.73, P < 0.0001༉,and Prevotella༈r = 0.65, P < 0.0001༉ was associated with higher PAHs concentration. Then a redundancy analysis (RDA) was further performed to determine the multivariate relationship between microbiota in samples and the environmental variable-PAHs by R. Although Stomatobaculum and Selenomonas was associated with PAHs level, their abundance were very low. The RDA confirmed Prevotella was positively correlated with 1-OHPyr level(Fig. 6).
3.4 1-OHPyr are associated with metabolic profile in asthmatic children
We also detected the metabolic profiles in asthmatic and the control group by UPLC-Orbitrap-MS. The variables with both VIP score > 1.0 and P-value < 0.05 were identified as candidate biomarkers. The metabolites that were confidently and putatively identified in the samples were listed in STable 2. After mapping to KEGG, the results showed that most of differential expressed metabolites (DEMs) were involved in purine metabolism, amino acid metabolism and lipid and fatty acid metabolism. Purine metabolic pathway was significantly aberrant (P < 0.0001, Fig. 7), which was in consistent with the results from studies [19, 20]. Phenylacetaldehyde, L-3-Phenyllactic acid, Hippuric acid, 4-Hydroxybenzoic acid, and L-Tyrosine were aberrant, especially the accumulation of Phenylacetaldehyde, L-3-Phenyllactic acid and Hippuric acid, which indicated the activation of phenylalanine metabolism (P < 0.005). Hypotaurine, acting as antioxidant, involved in organic osmolytes, was increased in asthmatic group. These implied responses to the oxidative stress conditions induced by environmental factors [21]. Interestingly, the level of 2-hydroxyfluorene(2-OHFlu), the metabolite of fluorene, one of PAHs, in asthmatic group was 1.29 times than that in the control( VIP = 1.06, P = 0.005). Lipid and fatty acid metabolism was also obviously influenced shown in STable 3. Phospholipid metabolites such as CL, PC, PG, and PS was increased, decreased was PE and PIP2. Phospholipids are the major component of pulmonary surfactant, attenuating the surface tension of the alveolus. Lysophospholipids in the lung were increased as pulmonary inflammation occurred and involved in the development of pneumonia and asthma [22]. TG, DG, MG, free fatty acids was increased, but Linoleic acid, polyunsaturated fatty acid, PUFA was decreased. It has been shown that PUFAs have significant roles in inflammatory process on different diseases. Our data was consistent with [23], suggesting a weakened anti-inflammatory effect. In addition, valproylglycine, prolylglycine, valyl-hydroxyproline glycylprolylhydroxyproline was increased in the asthmatic group, which were the major components of collagen-derived dipeptides and may be risk markers of osteoporosis and bone injury associated with corticosteroid treatment. Reinke et al found that prolylhydroxyproline was correlated with inhaled corticosteroid [19]. It is noted that me melatonin metabolite was very lower in the asthmatic group than that in the control group. The activation of the immune system may lead to free radical production, which may be exacerbated by PAHs exposure, associated with decreased melatonin levels in inflammatory diseases, such as allergic disease, asthma[24]. We conducted RDA analysis between 1-OHPyr and metabolites (Fig. 8). Pearson correlation showed that 1-OHPyr was positively correlated with deoxyadenosine monophosphate (r = 0.86, P < 0.0001), which is involved in purine metabolism (VIP = 1.04, Fold change = 1.46).
{kind=link}