The tongue is an organ with complex physiological and social functions that are seriously affected by tissue defects after the radical resection of tongue cancer. Partial tongue resection has a great effect on HRQOL. The repair and reconstruction of tongue defects are very demanding, but their purpose is to reconstruct the appearance, eliminate dead space, and maintain the patient's ability to chew, swallow and speak[6, 9]. Pedicled flaps and free flaps are commonly used to repair tongue defects. However, some studies suggest that with the use of pedicle flaps, the mobility of the reconstructed tongue and the recovery of speech are affected by gravity causing tongue and pedicle drooping[10]. It is also suggested that the reconstruction of the flap may impair the function of the residual tongue tissue due to the introduction of nonmotile tissue [11]. However, consecutive studies have shown that to improve postoperative speech and swallowing functions and the postoperative HRQOL, free flap reconstruction is necessary for restoration of the tongue volume and better functional outcomes in patients who have undergone resection of more than half of the tongue volume[7, 12, 13, 14]. The functional recovery of patients with free flaps repair after the operation is better, which is beneficial to improve postoperative HRQOL in this study. With the development of microsurgery, all kinds of free flaps are used in tongue reconstruction. At present, RFF flaps[15, 16], ALT flaps[13, 17], LAF flaps [8, 18], perforator flaps from the lower leg [19 ]and DIEP flaps[20]are also utilized in tongue reconstruction. Postoperative speech function and swallowing function quality depend on the strength, volume, and flexibility of the remaining tongue and flap repair. No study has shown that any flaps is superior to the other flaps in tongue reconstruction [21]. Therefore, this study is the first comparative analysis of the functional results of tongue reconstruction with four kinds of free flaps after radical resection of tongue cancer.
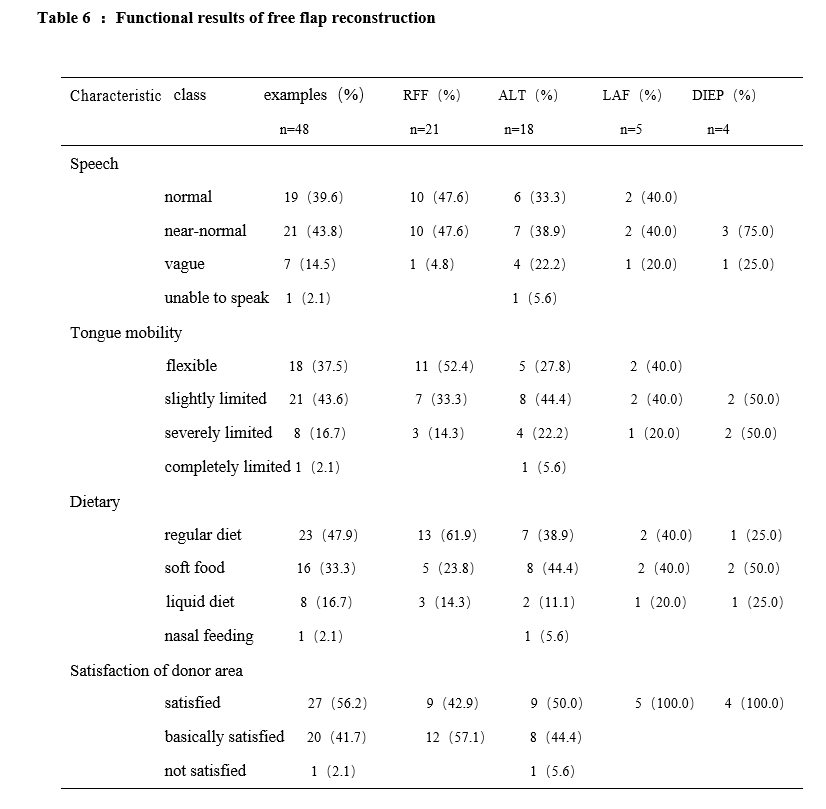
The RFF flap is still the main flap currently used for tongue reconstruction[12]. In this group of patients, 21 (43.6%) tongues were rebuilt with an RFF flap, which is also the main repair method. Postoperative functional evaluations revealed that after the operation, 47.6% of the patients had normal speech and 47.6% of the patients had near-normal speech. In 52.4% of the patients, the postoperative tongue flexibility was normal, whereas 33.3% of the patients had slightly limited postoperative tongue flexibility. Furthermore, 61.9% of the patients ingested a regular diet, and 23.8% of the patients received soft foods after surgery. The postoperative functional recovery was better in the RFF flap group than in the other three groups (Figs. 1, 2, 3). Thus, our study shows that RFF is still a suitable method for tongue reconstruction. The functional recovery of patients with tongue reconstruction using an RFF flap is satisfactory, especially when the tongue defect involves 1/3 − 1/2 of the organ; 13 (61.9%) patients of this study underwent repair of stage T1 and T2 defects. Therefore, for patients with tongue defects involving less than 1/2 of the organ, we tend to recommend the use of an RFF flap for tongue reconstruction. The main disadvantage of the RFF flap is that interception of the RFF involves cutting off the radial artery, which is the main artery for the forearm. This procedure can affect the sensation and motor function of the hand, and the concealment of the surgical wound is not ideal. Second, grafts are needed to block the donor area, and the scar is so apparent that it is difficult for many people to accept [22, 23]. In this study, only 9 (42.9%) patients were satisfied with the donor area postoperatively, which was the lowest level of satisfaction of any group (ALT, 50%; LAF and DIEP, 100%) (Fig. 4). Thus, the RFF flap procedure is not suitable for young people with high standards for appearance or for professionals with special requirements.
It is precisely because of some shortcomings of the RFF flap procedure that the ALT flap is widely used in tongue reconstruction, especially for a large number of tissue defects caused by the radical resection of advanced tongue cancer, as the RFF flap is thin, has insufficient in tissue, and easily forms scars that reduce the flexibility of the reconstructed tongue. In contrast, the ALT flap can provide a sufficient tissue volume [13, 24, 25]. In this study, 18 (37.5%) patients received an ALT flap for tongue reconstruction, which was the second most commonly used method. The postoperative functional evaluations revealed that 33.3% of the patients exhibited normal speech, 38.9% of the patients exhibited near-normal speech, and 22.2% of the patients exhibited vague speech after the operation. Furthermore, 38.9% of the patients had a regular diet, 44.4% had a soft diet, and 11.1% received a liquid diet; these percentages were slightly lower than those after the RFF procedure. We conclude that most of the patients treated with ALT flaps have advanced tongue cancer, that the defect after the operation is more significant, that the repair flap is thicker, and that the duration of flap atrophy is relatively long. In this study, 8 (44. 4%) patients received ALT flaps to repair T3 and T4 defects. An HRQOL study reported that the postoperative assessment time should be 12 months later as a critical factor [26]. In this study, the tongue function was evaluated six months after the operation. Fifty-five percent of the patients were satisfied and 44.4% of the patients were basically satisfied with the donor area—slightly higher percentages than those for the RFF flap. Therefore, we believe that for patients with advanced tongue cancer, in which the tongue body defect is subtotal glossectomy or even total glossectomy involving resection of most of the tongue body and tongue root, postoperative aspiration and swallowing are a serious problem, and the ALT flap is a better choice[ 27, 28].
In addition to studies on RFF and ALT flaps, there have also been reports of using LAF and DIEP flaps for tongue reconstruction. In this study, 5 (10.4%) patients received an LAF flap for tongue reconstruction, and 4 (8.3%) patients received DIEP flaps for tongue reconstruction; postoperative functional evaluations of speech function and swallowing function showed almost no significant differences between the RFF and ALT flap procedures. (Fig. 1, 2,3).However, the donor satisfaction was 100% (Fig. 4), which was also the most significant advantage of the LAF and DIEP flaps, both of which were perforating flaps, and the donor's vessels were not important functional vessels. The postoperative complications of the donor area were significantly reduced to the minimum, which was better than the corresponding results of the RFF and ALT procedures. We think that the LAF flap is thin and easy to shape, can even carry definite sensory nerves to partially restore nerve function, and has little effect on the donor area after the operation. However, it is necessary to recognize the thickness of the LAF flap, the large variation in the donor vessel and caliber, the short vascular pedicle, and so on, and thus the requirements of this microsurgical technique are higher. There is evidence that the average artery diameter is 1.1 mm (0.8 to 1.4 mm) and that the mean vein diameter is 1.2 mm (0.9 to 1.5 mm) [29,30.31].
For the DIEP flap, the blood supply of the flap mainly depends on the inferior abdominal artery, which is the branch of the external iliac artery. Blood is mainly supplied to the middle and lower part of the rectus abdominis muscle, and most of the segmental branches appear near the semicircular line, which is mainly the perforating branch of the musculocutaneous artery. The perforating branch whose diameter after penetrating the deep fascia is greater than 0.5 cm, is the application base of the DIEP flap[20, 32]. In clinical work, the advantages were as follows: (1) adequate tissue and blood supply; (2) preservation of donor muscles, fascia and nerves and prevention of donor area injury, complications and rectus abdominis atrophy [20, 32], with a shortened postoperative recovery time;(3) a flap that was not easily deformed (without muscle tissue) after the operation; (4) a concealed donor area, which was more in line with the aesthetic requirement; (5) a donor area and recipient area that could be operated on at the same time, which shortened the operation time;and(6)separation of the perforating branch from the intramuscular segment, which lengthened the pedicle and made the flap design more flexible and more compliant[20, 32].However, there are still some shortcomings in the DIEP flap procedure, such as a large variation in the perforating branch position and diameter, complicated steps during the operation, etc. Furthermore, the procedure is not suitable for obese patients; the DIEP flap is too bloated, and fat liquefaction may occur after the operation, so it is not suitable for tongue reconstruction.
In this study, while there was no significant difference in postoperative function, LAF and DIEP flaps could provide a sufficient tissue volume, a concealed scar, and fewer complications in the donor area, both functional and aesthetic, and could be used to repair the defects of advanced tongue cancer. The number of LAF and DIEP flaps in this study is too small. We believe that with the in-depth review of applied anatomy of LAFand DIEP flaps, the continuous improvement of prosthetic techniques by head and neck surgeons, the renewal and development of microsurgical techniques and equipment, and the popularization and application of modern imaging techniques, The application value and status of LAF and DIEP flaps in the repair of tongue cancer defects will be increase, and the role of them will become more important.
{kind=link}