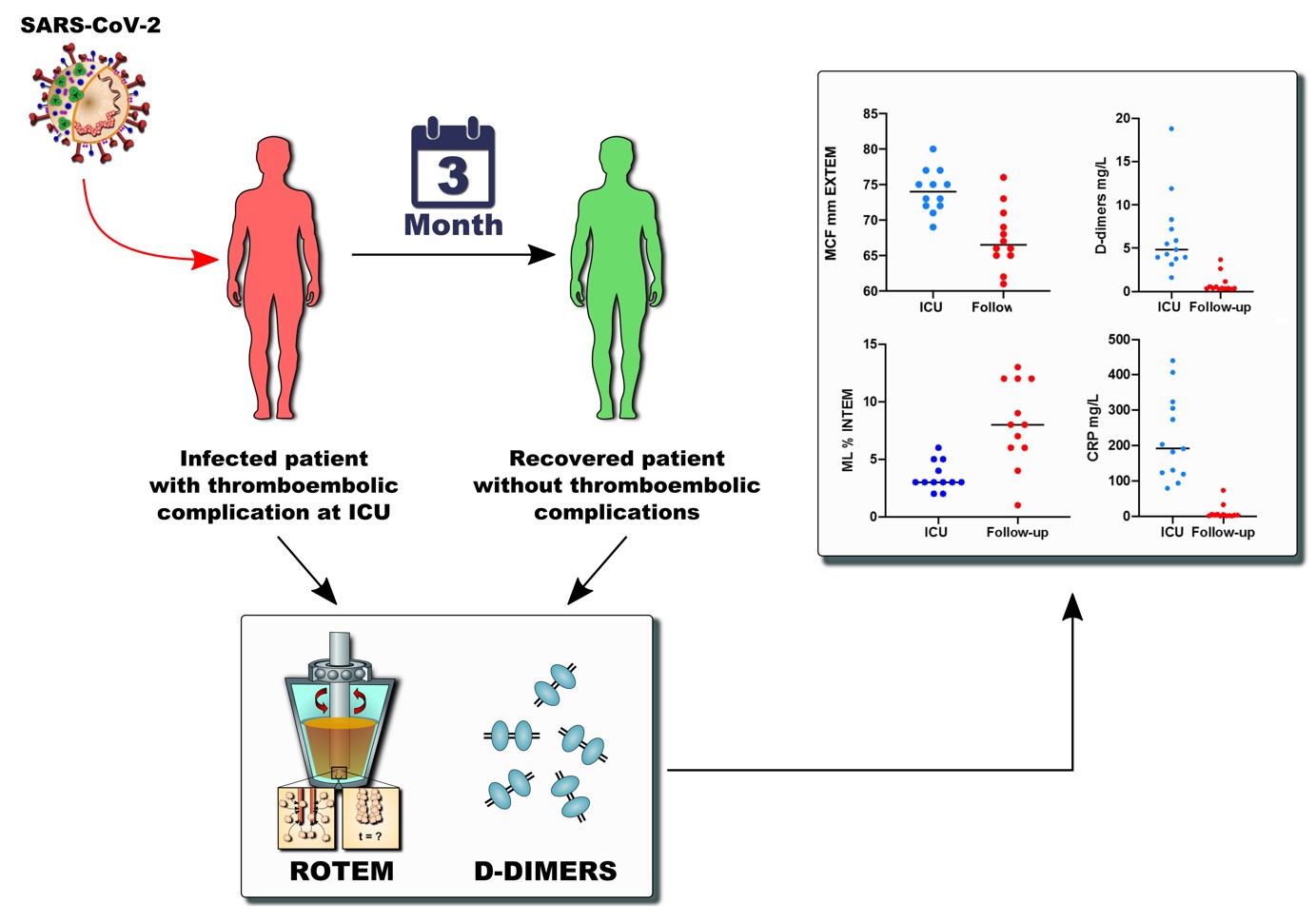
We report the data of thirteen critically ill patients with COVID-19, who initially required ICU admission with a severely hyperinflammatory and hypercoagulable state characterized by high levels of d-dimers and fibrinogen and a markedly increased clot firmness consistent with impaired fibrionolysis. While a hypercoagulable state was noted during their stay on the ICU, on their first visit in the ICU-follow-up clinic three months after discharge, they presented with normalized markers of inflammation and coagulation. Fibrinolytic activity and clot firmness had returned to normal values consistent with the reversible nature of the initial hypofibrinolysis. All patients analyzed showed normal d-dimer levels reflecting normalized turnover of the coagulation system also taken as surrogate of recurrence risks. Following normalization of laboratory values and viscoelastic parameters anticoagulation has been discontinued in all patients.
Venous and arterial thormbembolism contribute significantly to morbidity and mortality in COVID-197,8,9, 10,11,7,12,13. The nature of COVID-19 coagulopathy appears to be complex and the exact mechanisms still have to be elucidated. In contrast to septic coagulopathy thrombocytopenia seems to be a rare finding and only few patients with COVID-19 meet the criteria for disseminated intravascular coagulation 22
Ranucci and Panagida performed comprehensive coagulation analyses in critical ill patients with COVID-19 including viscoelastic testing and demonstrated increased clot firmness beside significant elevations in levels of d-dimers and fibrinogen-levels as reported by various other authors23–25 25. The amplitude of the d-dimer level was associated with increased mortality in several studies 26, 25. Spiezia et al. and Pavoni et al. have also recently shown severe hypercoagulopathy in critical-ill COVID-19 patients using viscoelastic testing. 27,28 Microthrombus formation in the lungs and various other organs has been described in autopsy series11,29 Microvascular injury associated with complement deposition might serve as a possible explanation as Magro et al reported in their study 30.
SARS-CoV2 can infect endothelial cells through the ACE2-receptor and cause endothelial damage and apoptosis 31. Endothelial injury resulting in substantial endothelitis together with dysfunction seems to play a crucial role in the induction of microvascular thrombosis in COVID-19 32
Panagida et al found diminished activity of fibrinolysis in their ROTEM-analysis. 23 Similar changes have been reported in septic patients and might indicate protective mechanisms employed to isolate intruding pathogens 33 34. One might interpret the persisiting fibrinolytic shutdown in COVID-19 as a consequence of the fact that there is no effective therapeutic agent to influence viremia until today and to protect the endothelial cells that are not only the target of SARS-Cov2 but also the key tissue regulating fibrinolysis. Impaired fibrinolysis has also been linked to the pathogenesis of ARDS in general 35 36
Continuosly reported high levels of inflammatory cytokines and infiltration of tissues with granuloctes and monocytes as demonstrated for lung tissue in autopsy using caspase-3 immunostaining probably also play an important role in the pathogenesis of coagulopathy and thrombophilia in COVID-19 32 37 with a particular impact on endothelial damage.
Tang et al demonstrated decreased mortality in COVID-19 patients with coagulopathy who were treated with unfractionated heparin compared to those who did not receive heparin 38 Heparin has anti-inflammatory effects and might mitigate capillary leakage and favorably influence the toxic effect of damage associated molecular patterns (DAMPS) and histones on the endothelium 39 40.
The American College of chest physicians (ACCP) and the American Society of hematology (ASH) recommended low molecular weight heparin (LMWH) in prophylactic doses in critical ill COVID-19 patients and in therapeutic dose if venous thromboembolism (VTE) occurred 16
Recent guidelines of the International society on thrombosis and hemostasis (ISTH) recommend either prophylactic or intermediate dosing of LMWH or UFH. 41
Given the high incidence of thromboembolic events many centers switched to intermediate dosing of anticoagulation instead of standard prophylaxis 13 42
As a consequence, our patients received unfractionated heparin with a target PTT of 50–55 (normal range aPTT 39 s) seconds as long as there were no thromboembolic complications. Patients with thromboembolic events received therapeutic doses of unfractionated heparin with a target PTT of 60–80 seconds. Patients who showed resistance to heparin and failed to reach the target-PTT within a reasonable amount of time despite adequate dosing, were switched to Argatroban for direct thrombin inhibition.
In contrast to individual parameters, viscoelastic methods like thrombelastography and ROTEM permit functional evaluations of whole blood aggregometry. Thus it allows evaluation of the different and complex coagulation phases including the initiation, formation and stabilization of a clot, and finally, clot lysis. Still endothelial function and the influence of soluble tissue factor have to be taken into account as they will not be represented in the results of the test. Not only bleeding diathesis as the classical indication for viscoelastic testing but also hypercoagulable conditions due to different diseases were examined in the past using ROTEM and states of hyper- and hypofibrinolysis could be reliably detected and characterized by viscoelastic tests 43,44, 33,45.
Our cohort presented with a significantly increased clot firmness on the one hand and severely impaired fibrinolytic activity represented by a maximum lysis of < 3% during their ICU-stay on the other.
The clot lysis parameter ML provides information on the fibrinolytic capacity and was successfully used in several studies to asses hyper-, or hypofibrinolysis. Lower values of ML provide evidence of existing hypofibrinolysis, while values above 15% are suggestive for hyperfibrinolysis. Nouigier et al reported in their recent study that critical ill patient with COVID pneumonia have an impaired fibrinolytic capacity which was associated with increased levels of PAI-1 and TAFI. 46 It has also been proposed that decreased activity of urokinase-type plasminogen activator and increased release of plasminogen activator inhibitor-1 might be the mediating mechanism of hypofibrinolysis, but data to support this further are scarce 47.
On their 12-week follow up visit, clot firmness and fibrinolytic activity had normalized in all patients. The significant increase of ML in the follow-up assessment indicates an appropriate regeneration or reversibility of physiologic fibrinolytic capacity.
To the best of our knowledge, this is a first study reporting follow-up data on the reversibility of coagulation abnormalities after COVID-19 infection including viscoelastic testing.
ACCP recommends to evaluate patients for extended prophylaxis after their hospital stay depending on their risk of bleeding. 16 ISTH states, that post discharge prophylaxis for 2–6 weeks should be considered 41. For patients after VTE, current guidelines recommend therapeutic anticoagulation for at least 3 months 41
Especially patients with high d-dimer values were found to be at high risk of post-discharge VTE independent of COVID-19 48 Around 60% of all VTE in medical patients occur in the post-hospital discharge period with a more than 5 times increased risk in fatal pulmonary embolism 49. Newer studies reported favorable risk-benefit ratios for extendend prophylaxis in medical patients 50
In conclusion our patients who suffered from thromboembolic events during their course of COVID-19 received therapeutic anticoagulation during their ICU stay and continuation was recommended for the first three months thereafter. Taking into account the grade of immobilization and the high levels of d-dimers, increased clot firmness and severely impaired fibrinolysis on viscoelastic testing, we recommended therapeutic anticoagulation in the patients without thromboembolic complications until reassesement during their first visit on the post-ICU-clinic.
On their 3 months follow-up visit all patients presented with normalized values of d-dimer, fibrinogen and viscoelastic testing. Inflammatory markers were also normalized. Since there were no signs of a persistent hypercoagulable state left and none of the patients suffered from a thromboembolic event after discharge we conclude that anticoagulation may be terminated no later than three months after discharge from the ICU.
Our study has several limitations. We report the data of a relatively small single center cohort of critically ill patients which may limit generalizability. Due to its retrospective nature it can only be hypothesis generating. Our presumptions have to be verified in a clinical trial focusing not only on coagulation profiles but also on clinical data such as rate of thromboembolic events and ideally survival. All patients received intermediate or full dose anticoagulation and an interaction with our laboratory and viscoelastic markers cannot be entirely excluded.
Furthermore, in the meantime between ICU discharge and follow-up, no control follow-ups were routinely performed or analyzed.
Moreover, we only performed anamnesis, clinical examination and screening ultrasound examinations as follow-up exams.. There were no clinical or anamnestic hints for pulmonary embolism but routine tests regarding asymptmomatic events were performed so no statements regarding asymptomatic pulmonary embolism can be made.
In summary, we found substantially limited fibrinolysis in acutely ill COVID-19 patients with normalization after three months.

{kind=link}