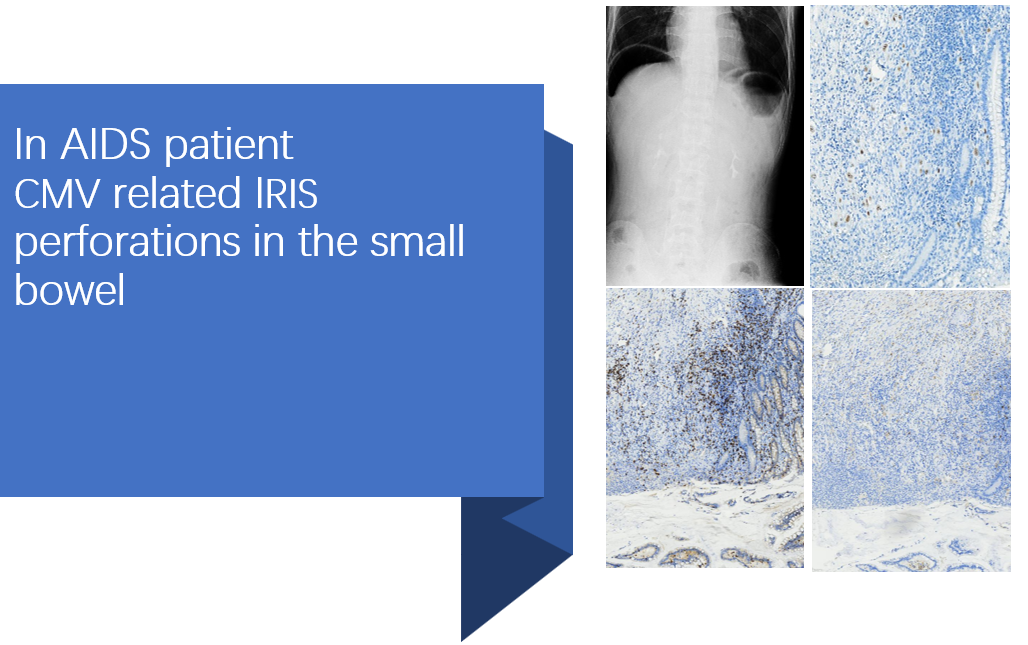
A 28-year-old Chinese man found several purple blue nodules on the face and neck for one month. He was detected positive antibody of HIV. His nadir CD4+ T cell count was 25cells/μL. After skin lesion biopsy, he was diagnosed with Kaposi’s sarcoma. The cytomegalovirus (CMV)-DNA load was 6.0×104 copies/ml. CMV antibody (IgM) was less than 8U / ml (0-18 U / ml), CMV antibody (IgG) was 12.3 U / ml (0-12 U / ml). No abnormalities were found in the funduscopic screening examination. Specific antibody of treponema pallidum (TP) was positive. Rapid plasma reagent ( RPR) test titer demonstrated 1:2 positive. The patient was treated with benzathine penicillin for three weeks. He started ART with the regimen of lamivudine (3TC) 300 mg daily, tenofovir disoproxil (TDF) 300 mg daily, and nevirapine 200mg twice a day. After 16 days of ART, the patient complained of fever and was admitted to our hospital. His highest temperature is 38. 9 centigrade accompanied by chills. He had no abdominal pain, diarrhea, and hematochezia. Blood routine test of the patient showed leukocyte 5.76×109/L (3.5-9.5 ×109/L), lymphocyte 1.29×109/L (1.1-3.2 ×109/L), granulocyte 4.04 ×109/L (1.8-6.3 ×109/L), hemoglobin (Hb) 87g/L (130-175g/L),and platelet (PLT) 348×109/L. The level of C reactive protein (CRP) was 88.7 mg/L (0-8 mg/L), and procalcitonin (Pct) was 0.66 ng/mL (0-0.05 ng/mL). Toxoplasma antibodies of IgG and IgM were negative. Liver function and kidney function were normal. His CD4+ T cell count has already increased into 75cells/μL. CMV-DNA load was 1.3×104 copies/ml. He was treated with intravenous ganciclovir. Ten days later, his fever disappeared. However, the patient presented persistent left lower abdominal pain which was spastic and tolerable. He had no abdominal distension, nausea, vomiting. The patient was conscious and had normal blood pressure(BP) 115/65mmHg, respiratory rate (R) 16 times / min, pulse frequency (P) 88 times / min and body temperature(T) 36.8℃. Abdominal examination showed that the abdomen was soft and flat, left upper abdominal tenderness, without rebound pain and muscle tension. Bowel sounds were 4 times / min. A standing x-ray of the abdomen in a tertiary level hospital revealed bilateral moderate intraperitoneal free air (Fig 1A). Intestinal perforation was considered. However, he and his family members declined surgical treatment and temporarily agreed with conservative treatment. Patients were given gastrointestinal decompression, proton pump inhibitors, ertapenem combined with levofloxacin, and nutritional support. Twenty four hours later, the vital signs were T 38.4℃, BP 110 / 70mmHg, P 130 times / min, R 18 times / min. The patient had tenderness pain in the left upper abdomen and right lower abdomen and whole abdominal rebound pain and muscle tension. We rechecked the standing x-ray of the abdomen found bilateral massive intraperitoneal free air (Fig 1B). Abdominal color ultrasound showed pneumoperitoneum and pelvic effusion. The images of abdomen computed tomography (CT) showed free gas with a low diaphragm (Fig 1C). Retested blood showed leukocyte 8.74×109/L, lymphocyte 0.65×109/L, granulocyte 7.96 ×109/L, Hb 103 g/L, and PLT 338×109/L. Alanine transaminase (ALT) was 102U/L (9-50 U/L) and creatinine (Cr) was 92 μmol/L (59-104 μmol/L). An exploratory laparotomy was performed. A total of 1000 ml of suppurative peritoneal fluid was cleared. Multiple perforations (40,50,65,140,240 cm proximal to the terminal ileum) were found at the anti-mesenteric border of small bowel. The largest diameter of holes was 1cm. Furthermore, multiple localized discolorations on the serosal surface of small intestine were presented indicating multiple deep ulcers (20,80,100,220 cm proximal to the terminal ileum). Partial enterectomy(35cm) and surgical repair of small bowel were performed. Histopathological showed the mucosa, submucosa and muscular layer were destroyed, neutrophil infiltration and granulation tissue formation were observed (Fig 2A). The serosa and myometrium showed pyogenic necrosis and a large number of neutrophils infiltrated (Fig 2B). There were intranuclear and intracytoplasmic inclusions typical of cytomegalovirus (Fig 2C). CMV enteritis was confirmed by hematoxylin-eosin staining and immunohistochemistry staining (Fig 2D). There were a variety of inflammatory cell infiltration, including MUM1 positive plasma cells (Fig 2E), CD68 positive tissue cells (Fig 2F), CD8 positive lymphocytes (Fig 2G), and a small amount of CD4 positive lymphocytes (Fig 2H). Kaposi’s sarcoma was firstly excluded. In order to identify other possible co-infectious pathogens, formalin-fixation and paraffin-embedded (FFPE) samples from a section of the resected bowel were sent to BGI PathoGenesis Pharmaceutical Technology (BGI-Shenzhen) for metagenomic next-generation sequencing (mNGS), which indicated CMV mono-infection without co-infections such as salmonella, tuberculosis, histoplasmosis, non-tuberculous mycobacteria, cryptococcosis, amebiasis, microsporidium, schistosomiasis. Intravenous ganciclovir at 5 mg/kg twice per day for another 2 weeks followed by 5 mg/kg/day for 1 month was applied. His CMV-DNA load was already less than 500 copies/mL. The patient had no fever and abdominal pain. He discharged home at 17 days after surgery and continued to take oral medication of ART without taking oral ganciclovir for secondary prophylaxis. One month after discharge, the patient was admitted again for abdominal pain and vomiting. The patient was conscious. The vital signs were T 36.5℃, BP 110 / 76mmHg, P 103 times / min, R 16 times / min. A standing x-ray of the abdomen did not show free gas and liquid gas level (Fig 1D). However, 24 hours later, the condition of this patient aggravated with a fever and decreased blood pressure. The vital signs were T 38.4℃, BP 90 / 48mmHg, P 140 times / min. Blood routine test showed leukocyte 5.52×109/L, lymphocyte 0.38×109/L, granulocyte 4.35 ×109/L, Hb 88 g/L, PLT 158 ×109/L. Amylase, lipase, myocardial enzyme, liver function and renal function were normal. We rechecked the standing x-ray of the abdomen showed visible dilated intestines and liquid gas level (Fig 1E). Adhesive intestinal obstruction and septic shock was diagnosed. The patient received meropenem, rehydration transfusion, dopamine, gastrointestinal decompression. Unfortunately, the patient's condition deteriorated and died at 55 days after surgery.
{kind=link}