Individuals with T2DM are with an increased risk of CVD which cannot be fully explained by elevated glucose[14]. Genetic risk factors contribute a lot to the pathogenesis of diabetic macrovascular complications, but its role has not been fully illustrated yet. In the present community-based case-control study, rs4845625 in IL-6R gene, and the interaction of rs184003 in AGER gene and rs4845625 in IL-6R were significantly associated with diabetic ischemic heart disease. Polygenic risk score calculated by summing the number of risk alleles of the SNPs located in the above two genes were also associated with the elevated risk of diabetic ischemic heart disease.
AGER is a multiligand cell surface receptor. Advanced glycation end products (AGEs) which is produced after high glucose exposure can bind to AGER. Their interaction has been implicated in the pathogenesis of atherosclerosis. In addition, HMGB1 (high-mobility group protein 1) and neutrophil-derived S100 calcium-binding family members (S100A8/A9/A11/A12, and S100B) were also ligands of AGER. After ligand binding, proinflammatory and procoagulant pathways will be activated. The rs2070600 was found to be significantly associated with diabetic ischemic heart disease in the current study. But after adjustments for covariates, the associations became null. The rs2070600 is located in ligand-binding V domain of the AGER gene, often referred to as Gly82Ser[15]. Genome-wide association studies (GWAS) showed that rs2070600 were strongly and dose-dependently correlated with sRAGE level in whites and blacks from Atherosclerosis Risk in Communities Study and Chinese population [6, 16]. Interestingly, although soluble-RAGE levels were found to be associated with diabetic complications in many researches, the association between rs2070600 and cardiovascular disease or other diabetic complications were not consistent. In Atherosclerosis Risk in Communities Study, the rs2070600 was not significantly associated with incident coronary heart disease or diabetes in both whites and blacks with a median follow-up of 20 years[6]. Gao et al. has found a significant association between rs2070600 and coronary arterial disease in 175 cases and 170 controls [17]. Meta-analysis found that the discrepancy may be attributable to ethnicity, subjects with rs2070600 risk allele were at higher risk of coronary arterial disease (CAD) in the Chinese population, rather than non-Chinese population. However, our study found the association between rs2070600 and diabetic ischemic heart disease was null. Another research also found rs2070600 was associated with the circulating levels of esRAGE but not with CAD in Chinese patients with T2DM [18]. These results might indicate that the association between rs2070600 and CAD may also be different in general population and T2DM patients.
Only few studies had demonstrated the association between rs184003 and cardiovascular disease. A hospital-based case-control study found rs184003 can significantly increase the risk of coronary artery disease (OR = 1.23, P = 0.008), and haplotypes C-T-G-G and T-A-G-T in AGER gene (rs1800625-rs1800624-rs2070600-rs184003) were associated with significant increases in risk for CAD[19]. In the current study, we also haplotypes C-G-T-A and A-G-C-A in AGER gene (rs184003-rs1035798-rs2070600-rs1800624) were significantly associated with diabetic ischemic heart disease. Although the rs184003 was significantly associated with diabetic ischemic heart disease in the current study, the associations became null after adjustments for covariates. To our knowledge, few studies illustrated the relationship between rs184003 and diabetic macrovascular complications. More researches are still need to validate our results. Given the fact sRAGE level were found to be significantly associated with CAD [20, 21] in many researches, the null association between AGER polymorphisms and diabetic ischemic heart disease in the current study indicated that sRAGE level could be served a marker of CAD, but not the a potential intervention targeting of reducing the burden of CAD.
Mendelian randomization analysis illustrated that IL6R signaling might have a causal role in development of coronary heart disease[22]. Previous meta-analysis demonstrated that rs2228145 and rs7529229 in IL6R could significantly reduce the risk of coronary heart disease[22, 23]. Although the meta-analysis constituting a large sample size, the data from Asian is insufficient. Chen et al. did not find an association of rs2228145 with coronary stenosis or acute myocardial infarction in the Chinese Han population[24]. Likewise, our current study, showed no association between rs2228145 and diabetic ischemic heart disease in Chinese population. The haplotype T-T-C-T-C (rs7529229-rs4845625-rs4129267-rs7514452-rs4072391) in IL6R gene and the rs4845625 was associated with diabetic cardiovascular disease in our study, and the association held after adjusting for potential confounders. The rs4845625 was found to be significantly associated with hypertriglyceridemia in Japanese population[25], and the T allele was associated with lower serum concentration of creatinine and increased eGFR[26]. Hypertriglyceridemia and chronic kidney disease (CKD) have common pathway leading to metabolic cardiovascular disease, like endothelial dysfunction, dyslipidemia, and inflammation[27]. Although there was seldom any study focus on the association between rs4845625 and diabetic heart disease, its association with triglyceride and kidney function might indicate the potential mechanisms of rs4645625 on diabetic ischemic heart disease.
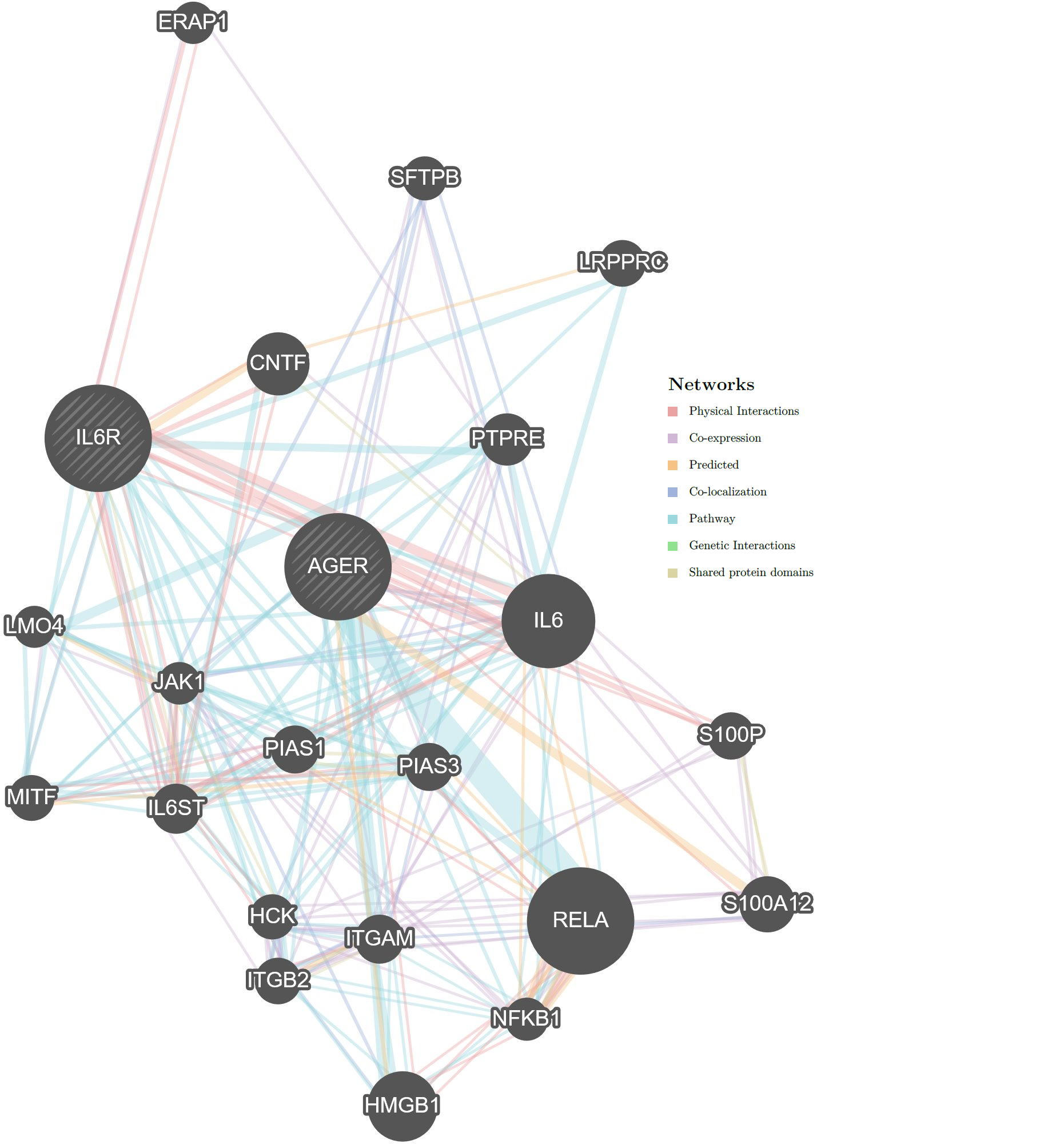
It has been found that, in response to hyperglycemia, AGER will be activated by S100A8/A9 on hepatic Kupffer cells, leading to the secretion of IL-6. IL-6 would subsequently bind to its receptor (IL6R) on hepatocytes to enhance the production of thrombopoietin, thereby regulating platelet production and resulting diabetes-induced thrombocytosis[28]. In the current study, we found that gene-gene interaction between AGER and IL6R would increase the risk of diabetic ischemic heart disease. We subsequently used GeneMANIA to construct gene network and predict gene function. IL6R and AGER have physical interactions with each other, and several pathways including NF-kB /RelA and JAK/STAT are involved in these interactions. Details were shown in Supplementary Figure S1. These interactions illustrated that the interaction of SNPs in IL6R and AGER was not only a statistical interaction, but also a biological interaction. To our knowledge, this is the first study aimed to identify interaction of AGER and IL6R gene, and our results provided a genetic evidence on the physiological mechanism of diabetic macrovascular complications. Whether the main effect and gene-gene interaction in these two genes could be used to predict the risk of diabetic macrovascular complications are still need to be validated by cohort study in the future. Although we found the significant interaction of AGER gene and IL6R gene, the association between circulating IL-6 and diabetic ischemic heart disease was null. This result indicates that the role of circulating IL-6 in the pathogenesis and development of T2DM cardiovascular complications is complex. The most common hypothesis is that local IL-6 production and dynamics of sIL-6R which indicated the activation of IL-6 trans-signaling pathway were more likely to affect the TPO production and macrovascular complications[28, 29].
In the current study, SBP, TC, LDLC level and the proportion of people with smoking and drinking habits were significantly lower in cases than in controls, which is not consistent with other researches. According to “2017 Guidelines for the prevention and treatment of type 2 diabetes in China”, diabetes patients have more stringent standards on blood pressure (BP) and blood lipid compared with health population, and diabetes patients with ischemic heart disease should quit smoking and drinking[30]. Diabetes patients might change their lifestyles and medication to maintain their BP or blood lipid at a lower level. Due to the case-control study design of the current study, we were not able to collect the lifestyle risk factors and blood sample before the incident of diabetic ischemic heart disease. However, the percentage of SBP, DBP, HDLC, LDLC, TG and TC in ideal range were significantly higher in control group compared with cases (P < 0.001, supplementary table S2). Due to the above limitation of our study, more longitudinal researches are still needed to demonstrate whether genetic variants will increase the incident of diabetic macrovascular complications. What is more, medication information was not included in the investigation. Given the fact that some antidiabetic medication, like SGLT-2 inhibitor[31], will reduce the risk of cardiovascular disease in diabetes patients, future researches considering antidiabetic medication are still needed to validate the genetic effect on diabetic macrovascular complications.
List of abbreviations
CVD, Cardiovascular disease
T2DM, Type 2 diabetes mellitus
AGER, Advanced glycation end products receptors
AGEs, Advanced glycation end products
IL-6, Interleukin-6
S100A8/A9, S100 calcium-binding protein A8/A9
FPG, Fasting plasma glucose
TC, Total cholesterol
TG, Triglycerides
HDLC, High-density lipoprotein cholesterol
LDLC, Low-density lipoprotein cholesterol
IHD, Ischemic heart disease
SBP, Systolic blood pressure
DBP, Diastolic blood pressure
PRS, Polygenic risk score
GMDR, Generalized multifactor dimensionality reduction
GWAS, Genome-wide association studies
Declarations
{kind=link}