Fluorescence-guided surgery is proposed as the next progressive iteration in cancer surgery, especially endo-laparoscopic operations.2,3 Notably, it is already impacting decision-making and step-sequencing in reconstructive surgery both of the gastrointestinal tract18 and other tissues.19 As well as a means to demarcate watersheds between perfused and non-perfused intestine, other uses include critical boundary identifications such as ureters20,21 and fascial planes22 by direct instillation. For cancer and draining lymph node identification, ICG has been placed peritumorally submucosally by endoscopic tattoo.23,24,25 In situ revelation of cancer including tumour margination however requires labelling pathology rather than physiology. While cancerous tissue can retain fluorescent agents, there remains a significant issue with false positive findings.26,27 Because of this lack of sensitivity, most research groups are now focusing on development of new cancer-selective agents although accuracy remains problematic.11,28, 29 ,30 Given that cancers likely act to accumulate agents in their vicinity differently to other areas that trap agents more passively, we thought to observe dynamically the processing of ICG by tumours under direct observation different to others who have focused on single point in time observations.
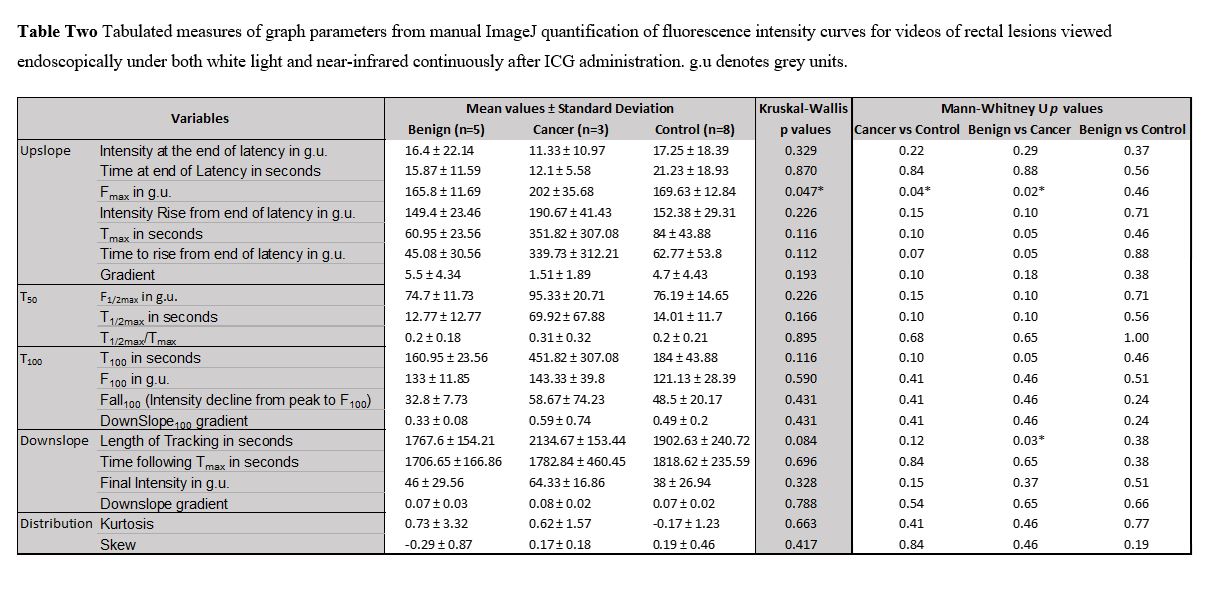
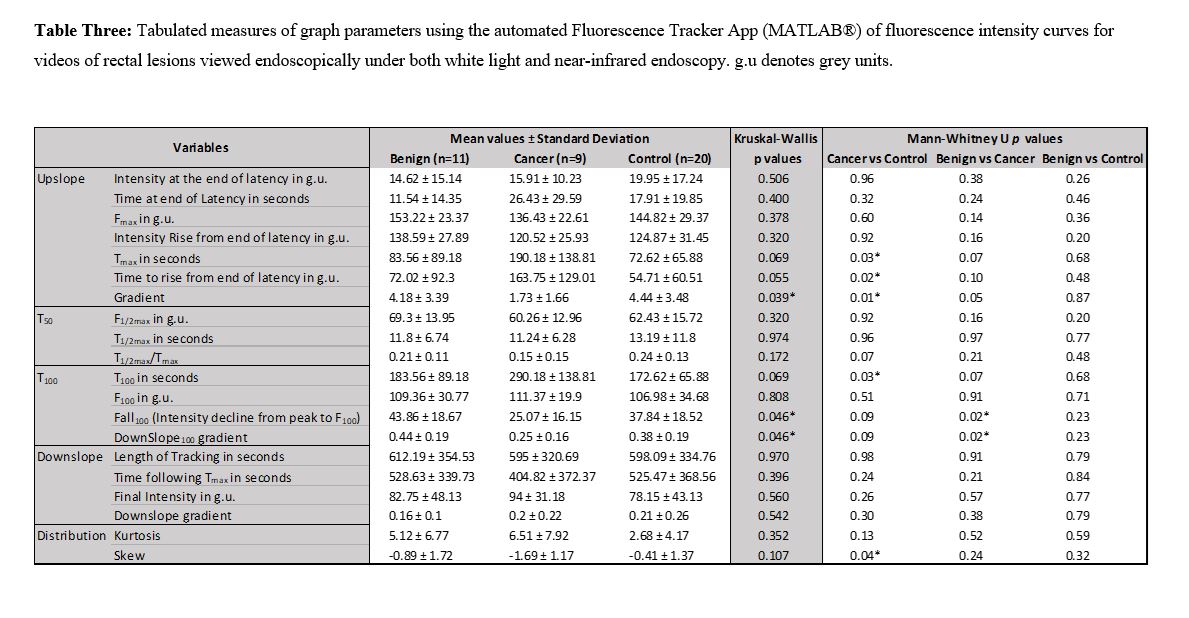
In this experience, visually obvious differential clearance patterns distinguish cancers from non-malignant tissues soon after agent administration and persist thereafter. While additional distinguishing parameters likely also exist and could be identifiable via longer videos enabling analysis of dye processing and efflux patterns and/or by using more sophisticated analytical methods, this initial work is revealing. Overall the fluorescence signal in tumours takes longer to peak and retains this intensity longer (consistent with impaired local pharmacokinetics compared with healthy tissue). Such distinct FI signatures could be visually noticed in both grey-scale, composite and threshold modes and could be quantified with post-hoc image data analysis. Manual intensity quantification allowed mathematical comparisons of the FI time patterns although such data generation was labour-intensive. Furthermore, episodic sampling (even at 1fps) made smoothing of data difficult while the background noise impaired statistical analysis. Automating feature detection, tracking and quantification enabled higher sampling rates (30fps) and so provided richer data for analysis with processing time being a function of computational ability rather than human labour. Automatic classification showed encouraging discriminate abilities even without prior annotation. Together these findings have great application for artificial intelligence methods.31
ICG accumulates quickly and can be effectively imaged with a variety of commercial cameras. Its attractiveness versus fluorescein lies in its responsiveness to NIR wavelengths (750-800 nm) which enables tissue penetration to approximately 1cm depth without cell damage (methylene blue may work similarly but is restricted in its intravenous licensing and has no CE or FDA-approved imaging device). Non-specific tumour uptake mechanisms include enhanced permeability and retention (EPR), aberrant gap junctions and dysregulated pinocytosis.32,33,34 Recent reports of similar behaviour of ICG at sites of secondary disease support this work21 and together the data are encouraging that malignant lymph nodes could behave similarly regarding uptake of circulating ICG. Although not the primary focus of this pilot experience, several positive nodes were visualized in situ during this study, though a larger cohort of patients would be needed to establish the generality of these observations. There are though many more patients who could benefit from an effective digital malignant discriminator for primary colorectal lesions (including those with significant polyps) however than there are presenting for surgery for recurrent disease. It is also likely that the ICG uptake mechanisms through cancer metabolics seen here are shared across other common cancers.
Cell-specific targeting remains of great interest for future advances in this area but a deep understanding of tumoural functional characteristics is necessary to inform the purpose and level of probe engineering needed. While cancer cell selectivity can be engineered in cell culture, tumour imaging in vivo can also encompass a variety of host:cancer interactions as well as additional cell signalling and response pathways. As ICG can be seen in this experience to passively concentrate in tumours it seems likely that so too will, at least in part, a “cancer-specific” agent. Furthermore, additional unrelated sites of inflammation35 or injury will equally be prone to incidental, unintended probe accumulation. This indicates that a relatively high rate of false positive findings may continue despite any additional tumour targeting features. Rigorous preclinical and clinical study controls are required to minimize heuristic mechanistic targeting assumptions. While long-in-advance (24–48 hours) administration of the fluorophore has been proposed to offset non-cancer signalling (and allow signal strengthening by agent concentration), a significant downside exists with respect to the unpredictability of operative timing and patient-to-patient pharmacokinetic variances.
An inbuilt synchronous and continuous dynamic quantification algorithm and screen display can be of use to all fluorescence imaging agents and could even enable synchronous use of multiple probes of different wavelength colours. Furthermore, while cell-surface or ligand-specific agents could be limited in applicability due to variance in intra and inter-tumour target expression, internalisation of ICG is governed by the tumour microenvironment, so it could perform similarly across a broad spectrum of cancers irrespective of tissue site or cell origin once the optimal real-time method for interpretative analysis is in place. Addition of cancer-specific targeting could still accelerate agent accumulation at the ROI following systemic distribution, enabling short-window observations with the greatest sensitivity and specificity possible within minutes. This would be a use for the operator more akin to episodic perfusion assessment with the added biochemical, biological and imaging complexity hidden. “Off-on” fluorogenic compounds are especially attractive for this purpose as their signalling only switches on when they arrive at the appropriate microenvironment.36
This study is of course limited by the small cohort studies although patients were recruited into the study without preselection. Fluorescence data is also dependent on the recording of the detected fluorescence signal. Video stability, suctioning, instrumentation and tumour desloughing impaired continuous tracking and required further user interaction. The distance and angulation of the camera as well as the depth of ICG have been found to influence the signal and need consideration in further protocols.37 Furthermore, while other surgical camera manufacturers offer similar systems for ICG visualization by NIR, camera design and performance investigation has shown previously significant inter-manufacturer variation between signal and ICG concentration (including the tendency of some systems to boost the images for human interpretation) which limits the generalizability of these findings until further (ongoing) validation is performed.38 While selection of the specific timepoints for analysis (e.g. 100 second post-peak timepoint) was somewhat arbitrary, they do provide milestones for statistical analysis enabling comparisons between lesions and adjacent healthy tissue as control. Statistical curve analysis is currently not calculated in real time and is limited to one curve per ROI. Simultaneous synthesis and dissection of multiple curves may further discern tumour heterogeneity. Although the automatic classifier diminished the differentiation ability of our metrics when compared to surgeon-based classification, better classification algorithmic methods may to some extent replace operator input. Other tracking algorithms exist and further software development may address field of view interruptions.
This endeavour has nonetheless shown that ICG with NIR-illumination is capable of delineating cancer in human patients in this specific test-case in a straightforward manner deployable within real-world surgical practice. The previous focus on spot readings may alleviate the need for concurrent injection and recording but has overlooked the potential for incorporating dynamic ICG flow patterns to improve confidence of interpretation. Equally incorporation of computer-assistance can help and even potentially replace the need for human observer visualization promising near real-time assessment of lesions during procedures with minimal user interaction as a ‘digital biopsy’ enabled through advances in computer processing, artificial intelligence and broad cloud-based datasets.39
{kind=link}
{kind=link}