We present analysis of the response to SARS-CoV-2 vaccination of 182 COV-AD participants sampled up to 2 months following their second vaccine dose (post V2 timepoint - median time from second vaccination: 45 days), 111 participants sampled 1 month before their third primary immunisation (pre V3 timepoint - median: 174 days from second vaccine, 17 days before third vaccine) and 161 participants sampled up to 3 months after their third primary immunisation (post V3 timepoint - median: 47 days from third vaccine). Demographic information for these groups are provided in Table 1. The overwhelming majority of participants (88.8-93.4%) in each group were receiving immunoglobulin replacement therapy for antibody deficiency. Between 59.3% and 63.3% of participants in each group received the AstraZeneca ChAdOx1 nCoV-19 vaccine for their initial two doses. 97.7% of participants received an mRNA-based third primary immunisation, 94.4% of them the Pfizer BioNTech 162b2 vaccine.
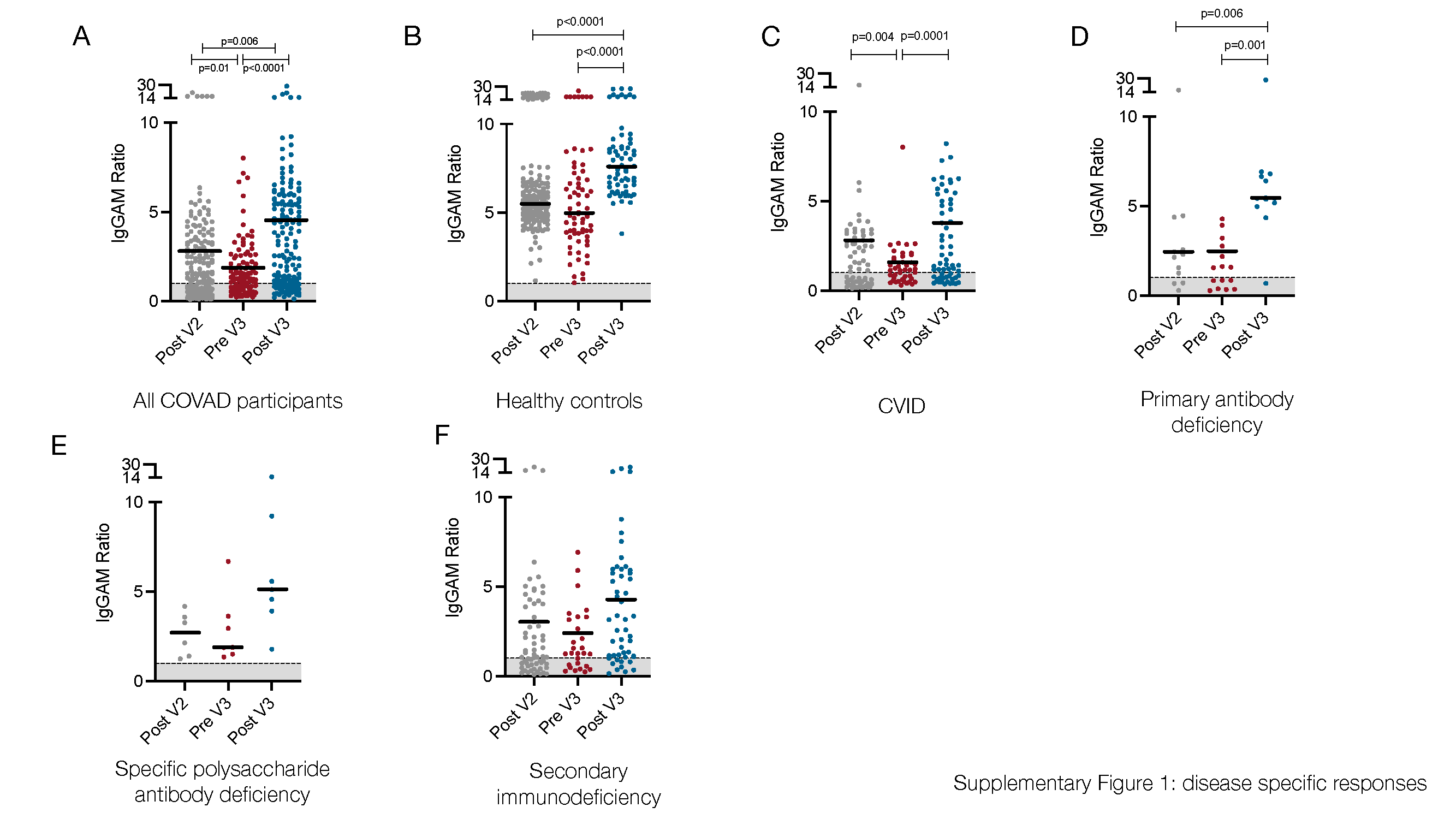
In the six month period following the second vaccine dose, anti-SARS-CoV-2 spike antibody levels, but not seropositivity, significantly decreased (2-way ANOVA, p=0.0002) (Figure 1A). A third primary immunisation significantly increased seropositivity in the COV-AD cohort (Seropositive %: Pre V3 - 61.4% vs. Post V3 - 76.0%, Chi Square 6.15, p=0.013) but the percentage of participants with detectable antibody responses remained lower than healthy controls, all of whom were seropositive, at all time points (Chi square: COV-AD vs healthy controls at Post V2, Pre V3 and Post V3; p<0.0001). A third vaccine dose also increased the magnitude of the antibody responses in COV-AD participants (2-Way ANOVA; Tukey’s multiple comparison test - IgGAM ratio: Pre V3 1.88 vs. Post V3 4.54, p=0.0007). However, in comparison to healthy controls, these responses were significantly lower at every sampling point (2-way ANOVA, p<0.0001) (Figure 1B, Table 2). A third vaccine dose increased seroprevalence and humoral responses in all major disease subgroups: CVID, primary antibody deficiency, SPAD and secondary immunodeficiency (Table 2, Supplementary Figure 1). Immunological correlates of post-vaccine seropositivity following the third vaccine dose were similar to those we have previously reported (5): vaccine responders had higher pre-treatment IgG level (mean IgG 3.7g/L vs. 2.02g/L, p<0.0001) and larger populations of peripheral blood CD19+ B cells (mean CD19 population 0.50x109/L vs 0.12x109/L, p=0.042).
Two doses of the Pfizer BioNTech 162b2 vaccine has previously demonstrated superior humoral immunogenicity in individuals with antibody deficiency compared to two doses of AstraZeneca ChAdOx1 nCoV-19 (5). In the 6 months following following V2, this superiority was maintained, but the effect lessened over time (2 way ANOVA; p=0.0011) (Figure 1A). At 6 months post V2, there was no significant difference in seroprevalence (AZ 56.1% vs. Pfizer 55.6%, NS) or the magnitude of the antibody response (IgGAM ratio: AZ 1.8 vs. Pfizer 1.58, NS) between recipients of the two vaccines. Furthermore, following the third primary immunisation, there was no significant difference in the percentage of seropositive individuals or the magnitude of the antibody response amongst individuals who initially received two doses of AstraZeneca and those who received two doses of Pfizer (% Seropositive: AZ 76.8% vs. Pfizer 73.6%, NS; IgGAM ratio: AZ 4.35 vs. Pfizer 4.63, NS) (Figure 1C). Prior PCR proven SARS-CoV-2 infection also did not significantly increase the magnitude of the serological response, although the numbers of patients with prior infection was low (Figure 1D).
Heterogeneity in the antibody response to vaccination was observed amongst individuals with primary and secondary immunodeficiencies (Figure 1E). Individuals with X-linked agammaglobulinaemia (XLA) did not mount an antibody response to vaccination, in keeping with the molecular mechanism underlying their immunodeficiency. Amongst the other major disease groups, individuals with CVID demonstrated the lowest post-third vaccine dose seroprevalence and lowest median antibody response following the third vaccine dose. In contrast, individuals with SPAD, who by definition have not responded to prior pneumococcal vaccination, all responded to COVID vaccination. (Table 2, Supplementary Figure 1).
Paired samples were available from 64 participants bled 1-2 months after their second dose and 1-2 months after their third dose (Figure 1F). Overall seroprevalence in these participants rose from 59.4% after V2, to 75.0% after V3 demonstrating the immunogenicity of a third primary vaccination in non-responders to the first two doses. Paired samples from the same participant were available from 37 participants before and after the third vaccine dose. Using ELISAs, these samples were analysed for levels of IgG directed against the original Wuhan SARS-CoV-2 spike protein and the B.1.1.529 SARS-CoV-2 variant of concern (Omicron) (Figure 1G and 1H). Seroprevalence of IgG antibodies directed against the Wuhan and Omicron spike proteins was 62.2% and 40.5% respectively prior to the third vaccine dose. Following third primary immunisation, the seroprevalence of antibodies directed against the Wuhan spike protein increased to 78.4% (Chi square 1.62, not significant) and significantly increased to 67.5% against the Omicron spike protein (Chi square 4.44, p=0.02), demonstrating the ability of a third primary immunisation to induce cross-reactive antibodies directed against dominant SARS-CoV-2 variant of concern in early 2022. However, seroprevalence against the Omicron variant amongst COV-AD participant remains significantly lower than healthy controls (COV-AD vs healthy controls: 67.5% vs 100%, Chi Square 22.2, p<0.0001). The functionality of the antibody response was investigated using live virus neutralisation assays directed against the Wuhan SARS-CoV-2 strain: third primary immunisation was associated with a significant increase in serum neutralisation capacity (median % neutralisation: Pre V3 44.8% vs. Post V3 99.8%, p=0.0479, n=14 paired serum samples) (Figure 1I).
T cell responses to infection and vaccination were measured by ELISPOT (Figure 2). Overall, T cell responses were detectable in 47.5% (n=47/95) of individuals after the second vaccine dose, 46.4% of individuals prior to their third vaccine dose (n=13/28) and 59.6% (n=28/47) of individuals after their third vaccine dose. Individuals with prior PCR-proven SARS-CoV-2 infection were more likely to have a detectable T cell response (Post V2: 94.1% vs 38.8%, Pre V3: 70.0% vs 33.3%, Post V3: 91.6% vs 48.6% - Chi Square p<0.05 Post V2 and Post V3) and that T cell response was quantitatively greater (Kruskal-Wallis 24.5, p=0.002; Dunn’s multiple comparison tests: Post V2 prior infection vs infection naive: p=0.0002. Post V3 prior infection vs infection naive: p=0.03) (Figure 2A). T cell responses were more frequently detectable in individuals with prior infection regardless of their vaccine schedule (Figure 2B). However, in SARS-CoV-2 infection-naive individuals, a greater percentage had a detectable T cell response at the V3 timepoint if they had received a heterologous third vaccine dose (i.e. two doses of ChAdOx1 nCoV-19 followed by an mRNA vaccine) compared to those who had received three consecutive doses of mRNA vaccines (heterologous vs homologous: 61.5% vs 11.1%, Chi square 6.81, p=0.009). There was no statistically significant relationship between the magnitude of the antibody response to vaccination and the presence or absence of a detectable T cell response (Figure 2C).
{kind=link}