The present review on the SMC was based on the review of manuscript published online and books using “SMC” or “Seasonal malaria chemoprevention” in google search and pubmed. A total of 94 free full text were available when cross checking between both google scholar and pubmed at the time of stopping the review. The manuscripts with only abstracts available were excluded as we couldn’t access to the full text. We then review subsequently the following: deployment and implementation progression, the impact of SMC on the prevalence of malaria cases in high-risk individuals, the factors affecting the effectiveness of the Seasonal Malaria Chemoprevention and the interaction of the SMC with and malaria immunity? The review was focused specifically on manuscript describing SMC in Sahelian Africa including as well few general SMC analysis mainly WHO (an one from East Africa), all represented in the references section. f
Quality and outcomes of the selected studies for review.
Although we sought out the bulk of articles on SMC with full texts, the reality of our review focused primarily on data collected in the Sahelian part of Africa where SMC is the WHO recommendation. Of course, we have used some data from Nigeria and Ghana, parts of which have a seasonal malaria transmission pattern. We believe that focusing the review on articles published on studies conducted in Burkina Faso, Mali, Niger, Senegal and Chad will essentially better answer the search for the effect of SMC on resistant genotypes or immunity that we are looking for because the essential at the moment of the WHO requirements and recommendations are focused in this area waiting as it seems to be the case that other countries are strongly concerned.
SMC deployment and implementation in Sub-Saharan Africa
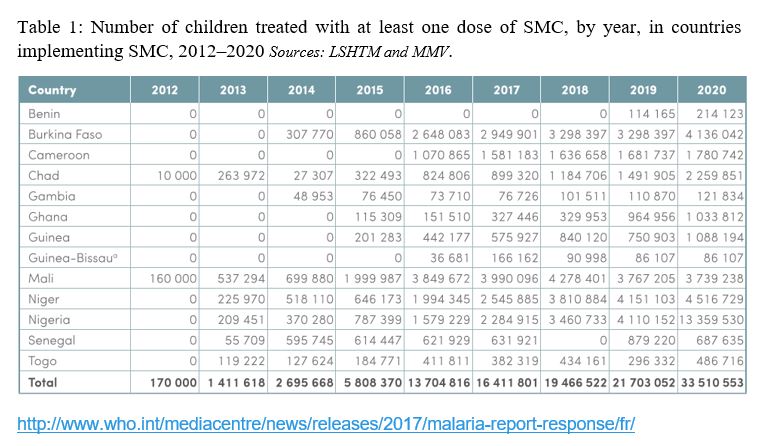
The implementation of SMC in Sahelian countries has been generally gradual from a pilot phase in the various countries to a full-scale phase to the entire population of concerned countries. By organizing the implementation in this way, the actors learn from the lessons, failures and then improve the progress in oil spot. This implementation process has been strongly supported by committed organizations (Medicines for Malaria Venture, Malaria Consortium, UNICEF, Global Fund, UNITAID, WHO, World Bank, PMI,) alongside with National Malaria Control Programs in Sub-Saharan Africa. This synergy remains today a winning combination in the implementation of SMC in Sub-Saharan Africa. Indeed, by bringing in their experience in program management, by building bridges between the different countries implementing this strategy and bringing additional financial and logistical resources, the scale up of SMC has been remarkable to reach the majority of eligible children in the Sahelian countries. Country like Burkina Faso, took about 6 years (2014 to 2019) to cover the country entire health districts (about70 health districts) with the support from Malaria Consortium, USAID, PMI, Unitaid, Global Fund, World Bank (figure 2).
This structural and sequential organization of SMC implementation is well illustrated by Malaria Consortium (figure 3) as the key to its success. It is important that this organizational approach is well respected by the parties implementing the strategy by putting in place procedures to better monitor planned activities. Although the WHO policy recommendation is for 4 monthly cycles, countries can set their own policies according to the local context. In that context 5 cycles are now implemented in several countries, including Burkina Faso and Nigeria, in areas where the peak transmission season is slightly longer. But the core of the strategy remains the 4 months of implementation. Countries such as Burkina Faso is now implemented 5 monthly cycles at scale across the southern half of the country where malaria transmission seems to be longer than 4 months with an early onset compared to the rest of the country. One of the expansion approaches of the SMC concern also the targeted ages with the option to extend above 5 years. There are some studies that have focused on older ages (11) with arguments related to the shift of the transmission curve in the tranche from 5 to 10 years. Senegal is a pilot country in extending the age target from 5 to 10 years. Confirmations of the interest of the extension of the age range are strongly awaited to further enlighten the scientific community on the cost-benefit of this extension. In addition, the potential benefit of expanding the age group eligible for preventive treatment needs to be weighed against its potential risks, including development of drug resistance and/or the risk of hindering acquisition or maintenance of immunity. However, WHO Technical Advisory Committee felt that any adjustment should be tailored to the needs of each country and its context. This is especially important as countries should be supported to develop or revisit their strategies for greater effectiveness.
Impact of SMC on the prevalence of malaria cases in high-risk individuals
Pilot studies as a proof of concept of the SMC strategies
To confirm SMC as a strategy that can positively influence the prevalence or incidence of malaria in a population of children at risk of malaria, pilot studies were conducted mainly in Burkina Faso, Mali and Senegal, under the known names of intermittent preventive treatment in children. These studies, considered to be the "ancestors" of the SMC, involved more than 3000 children in each of these countries. The results generated from those studies allowed WHO to recommend the strategy for scaling up in the Sahel while the following should be noted.
In Senegal, Cissé et al. from the first intermittent preventive treatment study in children, showed 86% reduction of malaria incidence among children who received seasonal intermittent preventive treatment (12). A study in Mali showed an incidence rate of malaria disease per 1,000 person-months during the first 12 months of 3.2 episodes in the treatment group vs. 5.8 episodes in the control group with age-adjusted Protective Efficacy (PE) of 42.5%; [95% CI 28.6%–53.8%]. However, when considering the first 16 week of the follow up the age adjusted, PE was 67.5% [95% CI 55.3% – 76.6%] (13).
During the same period from a study conducted in parallel in Burkina Faso the incidence of malaria, defined as fever or history of fever with parasitaemia ≥ 5,000/µl, was 2.88 (95% confidence interval [CI] 2.70-3.06) per child during the intervention period in the control arm versus 0.87 (95% CI 0.78-0.97) in the intervention arm with a protective efficacy (PE) of 70% (95% CI 66%-74%) (p<0.001). This study showed a reduction of 69% (95% CI 6%-90%) in the incidence of severe malaria (p = 0.04) and a 46% of reduction (95% CI 7%-69%) (p = 0.03) in the incidence of all-cause hospital admissions. Interestingly, the result confirmed a reduction of the prevalence of malaria infection at the end of the malaria transmission season by 73% (95% CI 68%-77%) (p<0.001) and that of moderately severe anaemia by 56% (95% CI 36%-70%) (p<0.001).
Evidences of SMC influence on the reduction of malaria incidence and prevalence in children under five
Children under five are at high risk of malaria in endemic areas and have typically been targeted for malaria control interventions, along with pregnant women (14). Based on the positive results of the above mentioned pilot studies, WHO has recommended that in high transmission areas, Sulfadoxine Pyrimethamine combined with Amodiaquine be given at least a month apart during four months (15). Several studies have shown a sharp decline of the risk of malaria infections in these risk groups through the use of intermittent preventive treatment (IPT) with sulfadoxine– pyrimethamine (SP) in infants (IPTi) (16,17), and by seasonal malaria chemoprevention with SP + amodiaquine (SMC/SP+AQ) in children between age of 3 months and 5 years (18–20). Modelling studies (21,22) indicate a strong effect of SMC, suggesting that it is a promising intervention, but the evidence for long term routine implementation needed to be documented. A study in Mali showed that exposure to at least one cycle of the SMC campaign had positive and statistically significant clinical effects on malaria and anemia in children aged 6–59 months. The risk of RDT-confirmed malaria was reduced by 44%. With a national prevalence over 35% in children under five during high transmission season (22), SMC has the potential for major public health impact in terms of morbidity, mortality and use of health services attributable to malaria (16). However, the effect measured in the study was lower than the 62% reduction in period prevalence measured in Burkina Faso during a routinely implemented SMC campaign (15). A previous study conducted in two Malian districts suggested a larger effect; SMC was associated with a 65% reduction in the odds ratio of being infected by Plasmodium falciparum (measured by microscopy) (23). In 2014 and 2015, a difference-in-differences approach in Burkina Faso was coupled in the analysis with propensity score weighting to control for observable and time-invariant non-observable confounding factors (24) . This study showed that SMC reduced the parasitemia point and period prevalence by 3.3 and 24% points, with protective effects of 51% and 62% respectively. SMC also reduced the likelihood of having moderate to severe anemia by 32%, and history of recent fever by 46%. Self-reported coverage for children at the first cycle was 83%. To our knowledge, with prevalence < 10% during the peak of the transmission season, this is the first time that malaria can be reported as hypo-endemic in a sub-Sahelian setting in Burkina Faso. SMC has great potential, and along with other interventions, it could contribute to approaching the threshold where elimination strategies will be envisioned in Burkina Faso (24).
In Mali in 2014, a study showed that prevalence of parasitaemia at the end of the high transmission seasonal was lower in areas receiving SMC (18%) than in areas not receiving SMC (46%) (25). In Ghana, Kweku et al. found 69% efficacy in terms of reducing malaria incidence (26). Clinical trials and meta-analyses have demonstrated the efficacy of SMC to reduce malaria incidence during the intervention period and parasitemia prevalence at the end of the transmission season and suggest a positive impact on all-cause mortality (19,27). Experimental studies have also found evidence of a lower prevalence of moderate to severe anemia, but this reduction was not always significant across trials (26,28). Monthly administration of SP-3AQ was found to be the drug regimen with the highest efficacy, (29,30). Data of a study suggest that seasonal malaria chemoprevention has the potential to avert several million malaria cases and tens of thousands of childhood deaths each year if successfully delivered to the populations at risk (4). The robustness of the design, and the congruency of the results over the different outcomes and analytical approaches, substantiate our assertion that SMC had a significant (clinically and statistically) positive impact on child morbidity in the study area (31).
This effectiveness of SMC has been strongly confirmed (Figure 4) by the large study conducted between 2015 and 2016 through the ACCESS-MCH project in seven West African countries (Burkina Faso, Chad, Gambia, Guinea, Mali, Niger and Nigeria), which assessed coverage, intervention effectiveness, safety, feasibility, drug resistance, and cost effectiveness (36). These findings, while supporting efforts of the scaling up SMC with high levels of coverage in west and central Africa, emphasize the need to set up a resistance monitoring system in view of the potential risks of selection of resistance to sulfadoxine-pyrimethamine and amodiaquine (36).
Factors affecting the effectiveness of the SMC
SMC Coverage
The SMC requires that children 3-59 months of age receive an antimalarial treatment for 3 consecutive days during the months of SMC. This is extremely important, as shown in early pilot studies (37), for the success of the preventive strategy. It is also important that coverage, which is an important factor in the success of the strategy, is sufficient to ensure good protection in the target population. This coverage rate of SMC at each round was defined as the proportion of the children aged 3–59 months at the time of SMC who received the 3 days’ treatment of that specific round. Full SMC coverage was defined as the proportion of children aged 3–59 months who received the complete 3-day treatment course during all four rounds of SMC (37).
A very good coverage will result in a substantial reduction in malaria cases and deaths in the target population. SMC high levels of coverage can be achieved through door-to-door delivery as assessed by in Malaria Consortium in Burkina Faso (38).
Although coverage is a key to the success of the SMC, the availability of drug supplies and the timing of cycles to coincide with the high transmission period would inevitably affect the effectiveness of this strategy. Under these conditions, planning in the implementation of SMC is of great importance in order to anticipate possible implementation problems. Previous implementation experiences have served and continue to serve for the better organization of SMC, especially for countries that are just starting to implement SMC. And the role of partners such as MMV, Malaria Consortium and others in the organization of the different actors involved and in the consolidation of achievements in perfect synergy is of paramount importance in the success of the SMC.
Molecular markers of resistance to sulfadoxine -pyrimethamine (Pfdhfr Pfdhps)
During their evolution, the microorganisms have been able to thwart the traps set for them by the environment and especially their host (immunity and use of anti-infectious molecules). The emergence and spread of antimalarial drug resistance represent a serious public health problem. Plasmodium falciparum is now resistant to all antimalarials used even in the latest marketed as artemisinin-based combinations (32).
Then in the context of large implementation of antimalarial drugs chemoprevention Sulfadoxine-Pyrmethamien (SP) combined with Amodiaquine, as is currently the case with SMC in the African Sahel region, malaria parasite is under deep drugs and subjected to resistance. As previously defined, antimalarial drug resistance corresponds to the ability of a parasite strain to survive and/or multiply despite the administration and absorption of a drug in doses equal to or higher than those usually recommended but within the limits of tolerance of the subject (33). Pfdhfr (Plasmodium falciparum dihydrofolate reductase) and Pfdhps ( Plasmodium falciparum dihydropteroate synthetase) are membrane genes whose mutations confer plasmodium resistance to antimalarial drugs.
Previous studies have shown that SMC would affect the prevalence of resistant strains of the parasite through the evaluation of molecular markers of resistance. Obviously in the context of SMC, the mutations concerned are carried by the pfcrt (Plasmodium falciparum chloroquine resistance transporter), pfmdr1(Plasmodium falciparum multidrug resistance 1), dhfr (dihydrofolate reductase), dhps( dihydropteroate synthetase) genes. In that case, epidemiological monitoring of susceptibility to SP can be estimated by measuring the prevalence in the parasite population of key mutations that serve as surrogate molecular markers of the clinical response to anti-malarials (5).The prevalence of parasites that carry the “quintuple mutant” genotype, both the triple mutant haplotype, Pfdhfr allele N51I/C59R/S108 N and the double mutant haplotype, A437G and K540E mutations of the Pfdhps gene are strongly associated with clinical failure of SP treatment (3). Parasites carrying 51I/59R/108N triple-mutant allele of pfdhfr and the 437G/540E allele of pfdhps are major contributors to SP treatment failure (34,35). In most West African countries, the pfdhps allele with the single mutant, 437G are common, but parasites with the triple mutant pfdhfr and the key 437G/540E substitutions are still rare. What remains of great concern to public health in Sub-Sahara region. Indeed strategies using Sulfadoxine -pyrimethamin as SMC or intermittent preventive treatment of women in the last two trimesters of pregnancy (IPTp) which still provide some benefit, could in the presence of high levels of this common quintuple genotype (36) be jeopardized. It is in the light of all these complexities that WHO recommends surveillance for these genotypes, and replacement of SP for IPTp when these quintuple mutant parasites reach prevalence greater than 50%. More recently, in East and Central Africa, parasites with a triple mutant pfdhps allele 437G/540E/581G have been observed to abrogate the benefits of IPTp with SP in some areas (37,38) . A study showed that the IRN triple mutant allele of pfdhfr was present in 57% of the clinical samples (5). The triple mutant pfdhfr is common in West Africa as reported in Burkina Faso and neighbouring Benin and Gabon in Central Africa (39,40). In most of the West Africa and likely reflects spreading of parasites that carry the imported pfdhfr Southeast Asian allele from East African sources (41,42). In many regions, clinical responses to SP are seriously compromised and SP is no longer recommended for treatment of malaria episodes. However, it has been difficult to determine whether the efficacy of SP for IPTp is similarly compromised. These uncertainties mean that decisions about whether to introduce SMC or IPTp as additional malaria preventive strategies are partly dependent on the local level of resistance to the antimalarial drugs being used (3,36).
Molecular markers of resistance to amodiaquine (pfmdr1 and Pfcrt)
The pfcrt and pfmdr are also known as membrane genes whose mutations confer resistance of the Plasmodium malaria parasite to antimalarial drugs. There are markers used to facilitate the prediction of the responses of parasites to chloroquine (CQ) and Amodiaquine (AQ), but also to mefloquine (MF) and lumefantrine (LUM). Resistance to AQ and its metabolite has been linked to mutations in Pfmdr1 and Pfcrt76T (43,44). It has been shown that parasites combining both the pfcrt 76T and pfmdr1 86Y mutations and those carrying the pfmdr1 86Y/184Y/ 1246Y triple-mutant haplotype are resistant to 4-aminoquinolines and associated with clinical failure with AQ treatment (34,37) with a possible negative impact on the SMC effectiveness. Selection of the pfmdr1 N86/F184/ D1246 haplotype has been also reported during treatment with artemether–lumefantrine (AL) and in infections with increased sensitivity to mefloquine and decreased susceptibility to lumefantrine (37). In addition parasites that carry 2 or more copies of the wild type allele of pfmdr1 are also highly resistant to both lumefantrine and mefloquine (45). In Niger, Sahelien country, the F184Y mutation was found to be the most frequent, with 37% of sequences displaying this mutation. The 86Y, 1042D and 1246Y mutations were less common, with prevalence of around 0.1. In the study region, almost all (88%) the parasites carried the NFD or NYD haplotype, reflecting the selection exerted by AL, the first line treatment in Niger. Parasites carrying the YYY form were not detected. The pfcrt sequences were not determined in this study, but other analyses performed in southern Niger during the same period showed that the wild-type CVMNK allele (amino acids 72–76) of the pfcrt gene was present in 85% of clinical samples (46). This is consistent with previous in vitro results, which indicated that the clinical samples from Niger respond adequately to other 4-aminoquinolines like AQ (41).
Effect of Sulfadoxine Pyrimethamine-Amodiaquine -based SMC on Plasmodium falciparum resistant genotypes
The combination of SP+AQ has been proposed as a scheme that can ensure both immediate efficacy and a prolonged effect by the SP having a half-lasting effect, all of which could help to inhibit the development of parasite resistance. Of course, this hypothesis is still discussed by specialists. However, the long-term sustainability of SMC will depend on the sensitivity of malaria parasites to the antimalarial drugs used (46). In the Lo et al study, the impact of the use of SP+AQ over the course of three years are measured, on an increasingly large scale, on the prevalence of molecular markers of resistance in characterizing the prevalence of mutation in pfdhfr and pfdhps genes, associated with resistance to SP, and genes pfmdr1and pfcrt, markers of resistance to CQ and AQ. Among children with parasitaemia at the end of the transmission season, the prevalence of mutation pfmdr1-86Y was higher among children that had received SMC. There was no strong evidence that the prevalence of other mutations, among infected children, was different in SMC and control areas (figure 5). However, despite the large sample size of these surveys, the number of positives was low and confidence intervals were wide due to reduced transmission during the study period. In each year, the overall prevalence of SP-resistant genotypes was lower in SMC areas, as a consequence of the marked reduction in prevalence of infection in areas using SMC (46). The presence of mutations on knowing pfcrt, pfmdr1, pfdhfr and pfdhps gene or the increase of their proportion, while demonstrated by authors in West or East Africa after implementing of SMC(47,48) does not necessarily lead to SP+AQ treatment failure, as the anti-malarial immunity of individuals must also be considered.
Surprisingly, resistance of P. falciparum malaria to the new artemisinin compounds involves others novel mechanisms corresponding to a quiescence phenomenon (49). We emphasize the continuing challenges and the imminent need to understand mechanisms of resistance to improve parasite detection strategies, develop new combinations to eliminate resistant parasites and prevent their global spread (50). These uncertainties mean that the sustainable implementation of the SMC as a major malaria preventive strategies will partly dependent on the local level of resistance to the antimalarial drugs being used and this could be challenging (3,36).
Could SMC impact malaria immunity?
Long-term malaria chemoprevention by SMC/SP+AQ even limited could impact on the development of acquired immunity, as tested using the Plasmodium falciparum antigens GLURP-R0 and AMA-1 in previous Ndiaye et al study (5). However, as highlighted other factors, not measured in this study, may interfere as well (2). The glutamate-rich protein (GLURP) is an exoantigen expressed in all stages of the Plasmodium falciparum life cycle in humans. Anti-GLURP antibodies can inhibit parasite growth in the presence of monocytes via antibody-dependent cellular inhibition (ADCI), and a major parasite-inhibitory region has been found in the N-terminal R0 region of the protein (51); and AMA1 is an integral membrane protein of merozoites and sporozoites and has a central role in parasite invasion of erythrocytes and potentially hepatocytes that can be inhibited by anti-AMA1 antibody (52,53). A study in children under 10 years of age living in areas where SMC/SP+AQ implemented for 3 years in comparison with an area without SMC showed that for both Plasmodium falciparum antigens GLURP-R0 and AMA-1, total IgG response were higher in the district without SMC implementation. Similar results were found in Senegal by Boulanger et al. (54) where they showed that children receiving SMC had a slightly lower level of anti-Plasmodium schizont antibodies compared with non-treated control children after 8 months of implementation. Thus, the lower falciparum-specific antibody level noticed in the districts with SMC/SP+AQ most likely represent a lower development of acquired immunity towards malaria, and may be directly due to the SMC strategy (2). It is clear that in areas where malaria is highly seasonal, this strategy needs to be renewed each year to avoid a resurgence of malaria, while promoting the use of other antimalarial interventions (10). It is also important to stress that the reduction in immunity observed in antibodies to malaria antigens after chemoprophylaxis, may simply represent less parasite exposure rather than an actual loss of protective immunity as highlighted in previous studies (43,55). In Ghana, antibodies against various Plasmodium falciparum antigens were significantly lower in children treated once with SP than in controls (56). Thus, despite its beneficial impact, mass implementation of SMC raises concerns on whether naturally acquired immunity in treated individuals develops as in untreated ones (whether there is a rebound effect). The long-term effect of SMC/SP+AQ on immunity development in areas where this strategy has been routinely used for several years is not well documented (2). However, in the particular context of malaria, we need to balance the short-, medium- and long-term benefits and risks on malaria disease control in order to make the best decision for the health of children in sub-Saharan Africa.
Although there are still some concerns of the impact of SMC on the malaria immunity, there are still positive points that needs to be highlighted such as those linking SMC with greater weight gain or improvement of malnutrition indices (28,57,58). This remains an important point. Indeed, child malnutrition, and particularly stunting, may down-regulate the anti-Plasmodium falciparum Ab response, both in terms of prevalence of immune responders and specific IgG Ab levels.
Limited coverage of SMC in children by absence during the rainy season
Local contingencies may have reduced the adherence to SMC during its implementation and, consequently, limited its effectiveness in the specific area. Indeed, in a previous study assessing coverage of the SMC in children, self-reported coverage for the first cycle of the round was 76% and 83% at the household and individual levels (children < 5 years), respectively (59). This study found that coverage for children was 100% at the first cycle, then gradually decreased to 69% at the fourth cycle. Several factors could explain the limited coverage for households and for children, notably their absence during the rainy season. Indeed, it is common for some household members to spend all day in the fields. Some even leave their homes and temporarily live in shelters closer to the fields (59). Also, it is common for young children to stay with their mother during the day and accompany her wherever she goes. This could explain why, even if a household was visited, some children did not receive SMC treatment.
{kind=link}