2.1 The prevalence of LPR2 somatic mutation in pan-cancer
We analyzed LRP2 mutations in whole exome sequences of 10,953 patients from 32 different cancer types. We identified 797 patients with LRP2 mutations.The mutant frequencies in different tumors was significantly different, with the higher LRP2 mutation in melanoma (28.18%), uterine carcinosarcoma (17.99%) and lung squamous cell carcinoma (16.32%) (Fig. 1A). In additon, of the 797 LRP2 mutations, 651 (81.68%) were missense mutations, 100 (12.55%) were truncating mutations, 38 (4.77%) were splice site mutation and 8 (1.00%) were inframe mutation. These mutation appeared in a dispersed manner throughout the sequence and 3D protein structure (Fig.1B).
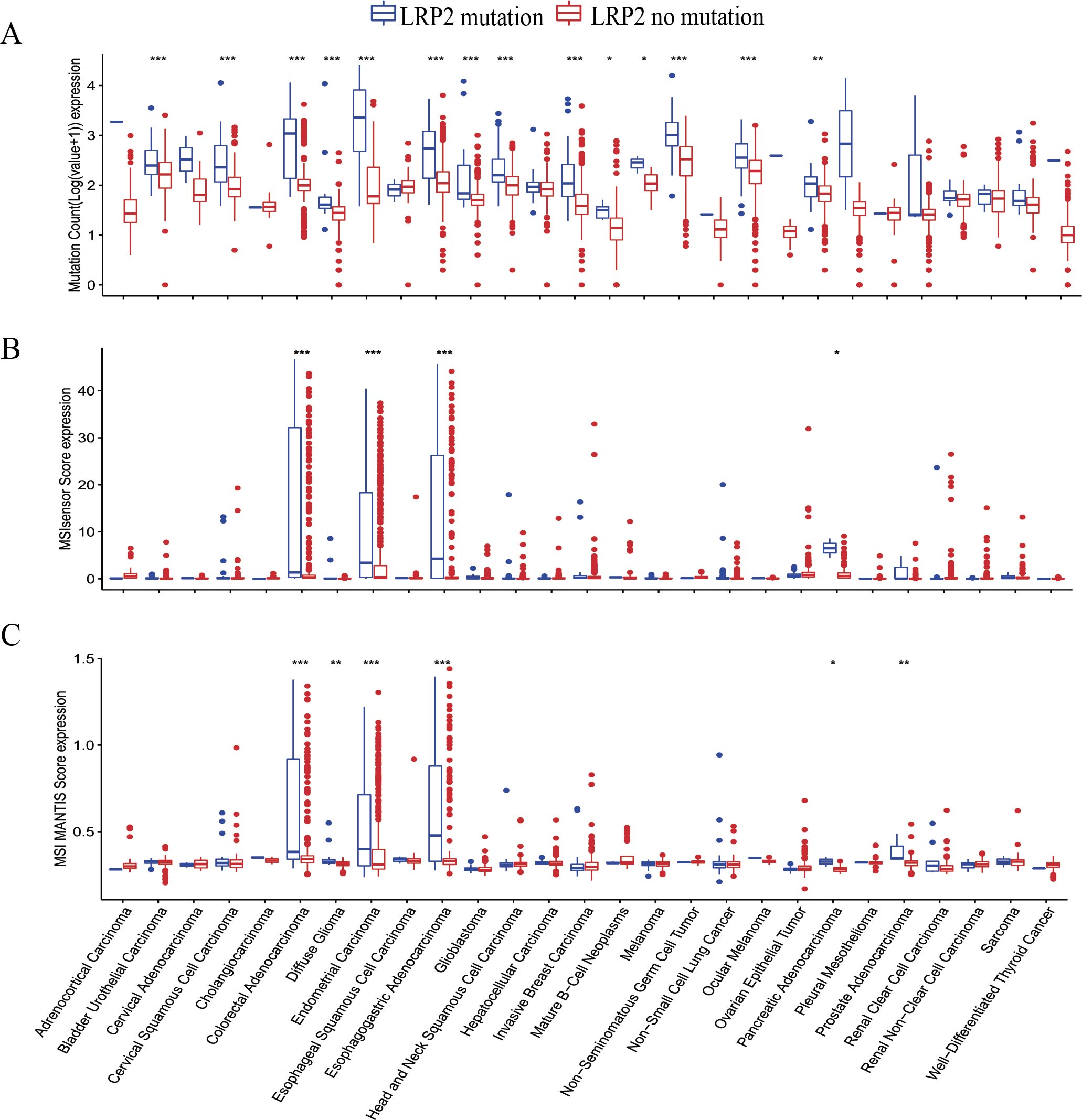
TMB has been shown to be a useful biomarker for ICIs selection of some cancer types; high TMB in tumors favors the infiltration of immune effector cells, and antitumor immune response [18]. In TCGA cohort, there was a significant difference between TMB and various muation types (truncating mutant, missense mutant and multiple mutations) (Fig.1C). Then, we explored TMB level in different tumors. The results showed that among bladder urothelial cancinoma, rectal adenocarcinoma and endothelial carcinoma, patients with LRP2 mutation had significantly higher TMB level as compared to that without LRP2 mutation (Fig.S1A). MSI has emerged as a major predictive marker for the efficacy of ICIs over the last few years [19]. MSIsensor is an effective tool to obtain MSI status. The results showed that patients with LRP2 mutation had a higher MSIsensor scores than that without LRP2 mutation in pan-cancer analysis ( P < 0.001) (Fig.1C). MSIsensor stratified by LRP2 mutation status showed that there was a significant difference between MSIsensor score and missense mutant and multiple mutations. To further vertify the association between LRP2 mutation and MSI status, we also examined the difference of MSI MANTIS scores between patients with LRP2 mutant and without LRP2 mutation. The results showed that MSI MANTIS scores in patients with LRP2 mutant were significantly higher than that without LRP2 mutation (Fig.1C). Then, we analyzed the MSI level among different tumor types. The results exhibited that MSIsensor and MSI MANTIS score were higher in patients with LRP2 mutation than those without LRP2 mutation in colorectal adenocarcinoma, endometheal carcinoma and esophagogastric adenocarcinoma (Fig.S1B-C).
MSH2, MSH6, MLH1, and PMS2 play a critical role in the process of mismatch repair (MMR). Any mutation in these four MMR genes may lead to MSI-H [20-21]. Here, we investigated the co-occurrence pattern of these four MMR mutant genes and LRP2 mutations (Fig. 1D). Compared with patients without LRP2 mutant, patients with LRP2 mutant harbored more MMR mutant (MSH6, 1.77% vs 12.2%; MSH2, 1.78% vs 10.78; MLH1, 1.60% vs 9.64%; PMS2, 2.25% vs 10.88%). In addition, we also found that LRP2 mutation was associated with common tumor-related sigaling pathways, such PTK/RAS/PI3K, p53 and RB signaling pathways (Fig.1E) and homologous recombination repair genes (Table.S1), suggesting that LRP2 gene may regulate tumor through synergy with other mutant genes. Meanwhile, the top genes mutation with LRP2 mutation included WWOX, OSBPL11, and SNX4, showed in Fig.1F.
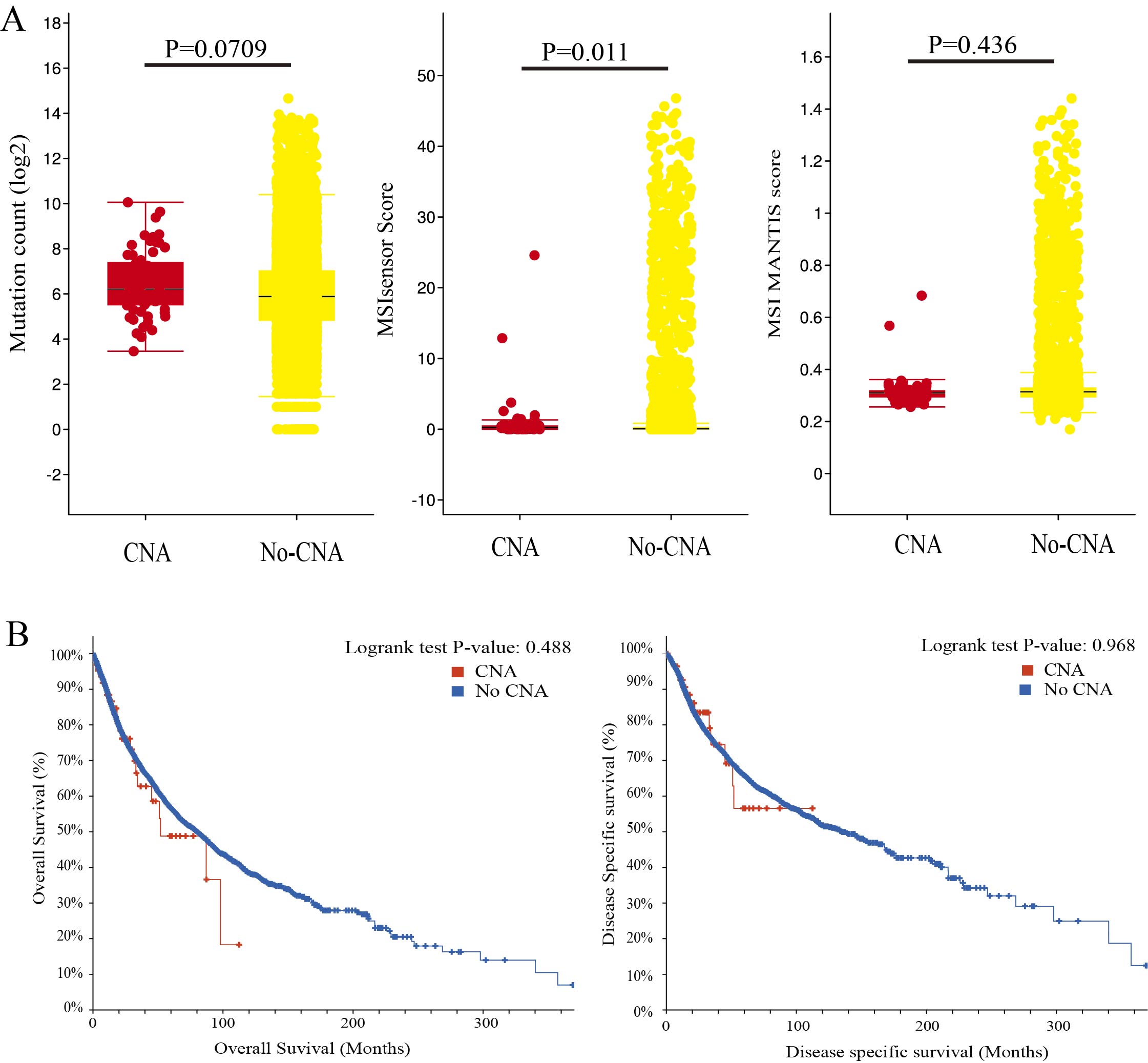
Then, we evaluated the effect of LRP2 on prognosis in pan-cancer analysis. The results showed that there was no significant difference in overall survival (OS) (P = 0.405), disease-specific survival (DSS) (P = 0.129) and progress-free survival (PFS) (P = 0.849) between patients with LRP2 mutantion and patients without LRP2 mutation (Fig.1F). The prognosis and survival for tumor patients in TCGA cohort were independent of LRP2 mutant status. Then, we compared the effect of LRP2 mutation on prognosis among different tumor types. The results showed that LRP2 mutation was associated with a better prognosis in endothelial cancer (OS, p<0.001), bladder urothelial cancinoma (OS, p=0.0061) and brain lower grade glioma (OS, p<0.0293) (Table.S2). In addition, we also examined the features of patients with CNA of LRP2 (Fig.S2). A total of 64 patients were idendified as 45 amplification and 19 deep deletion. The results showed that the CNA of LRP2 was not related to TMB level (P = 0.0709), MSI MANTIS scores (P = 0.436), OS (P = 0.488) and DSS (p=0.986). The outcomes indicated that LRP2 mutation was the main type in genomic alterations of tumors.
2.2 Relationship of LRP2 mutation with tumor microenviroment and immunotherapy
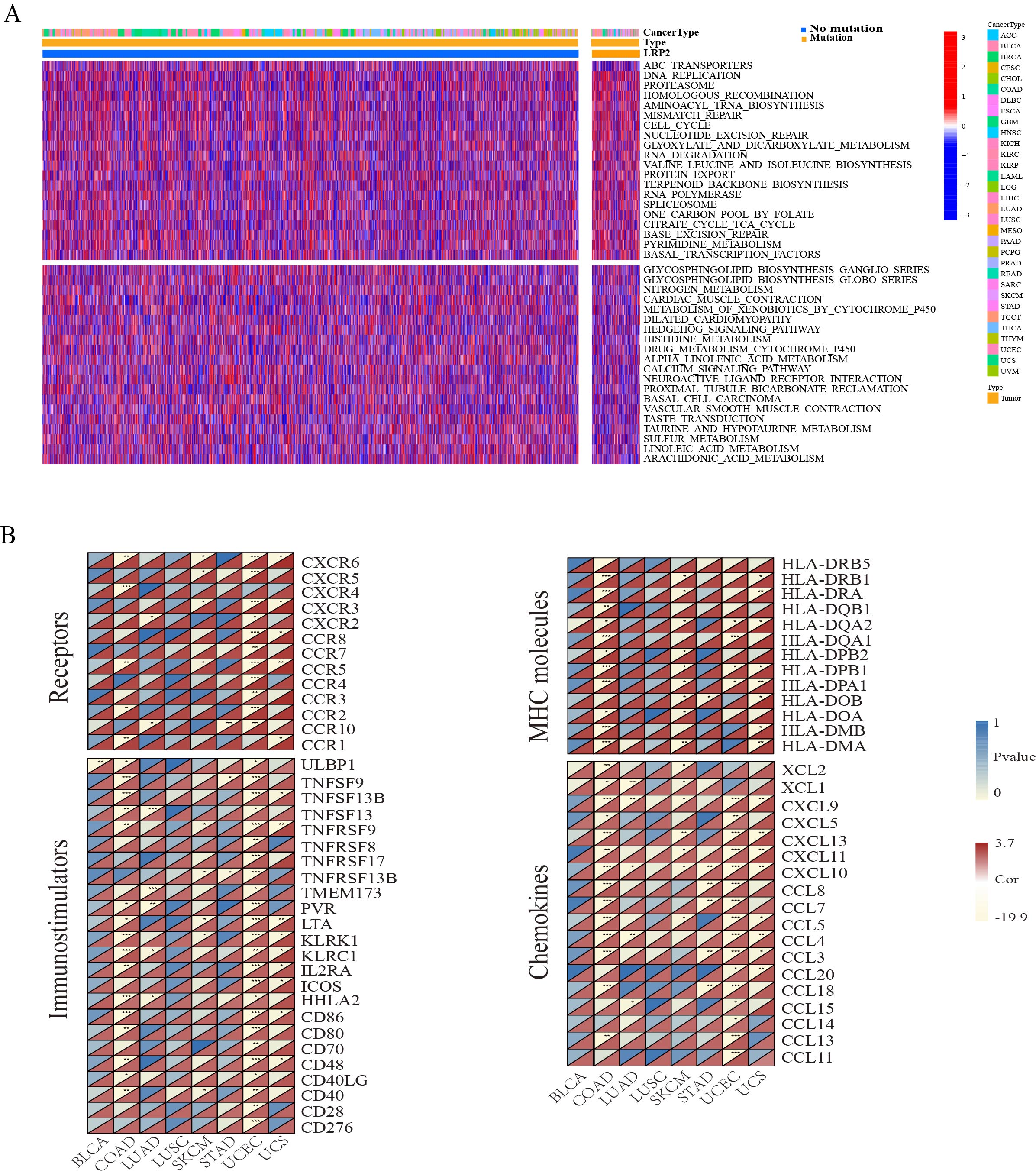
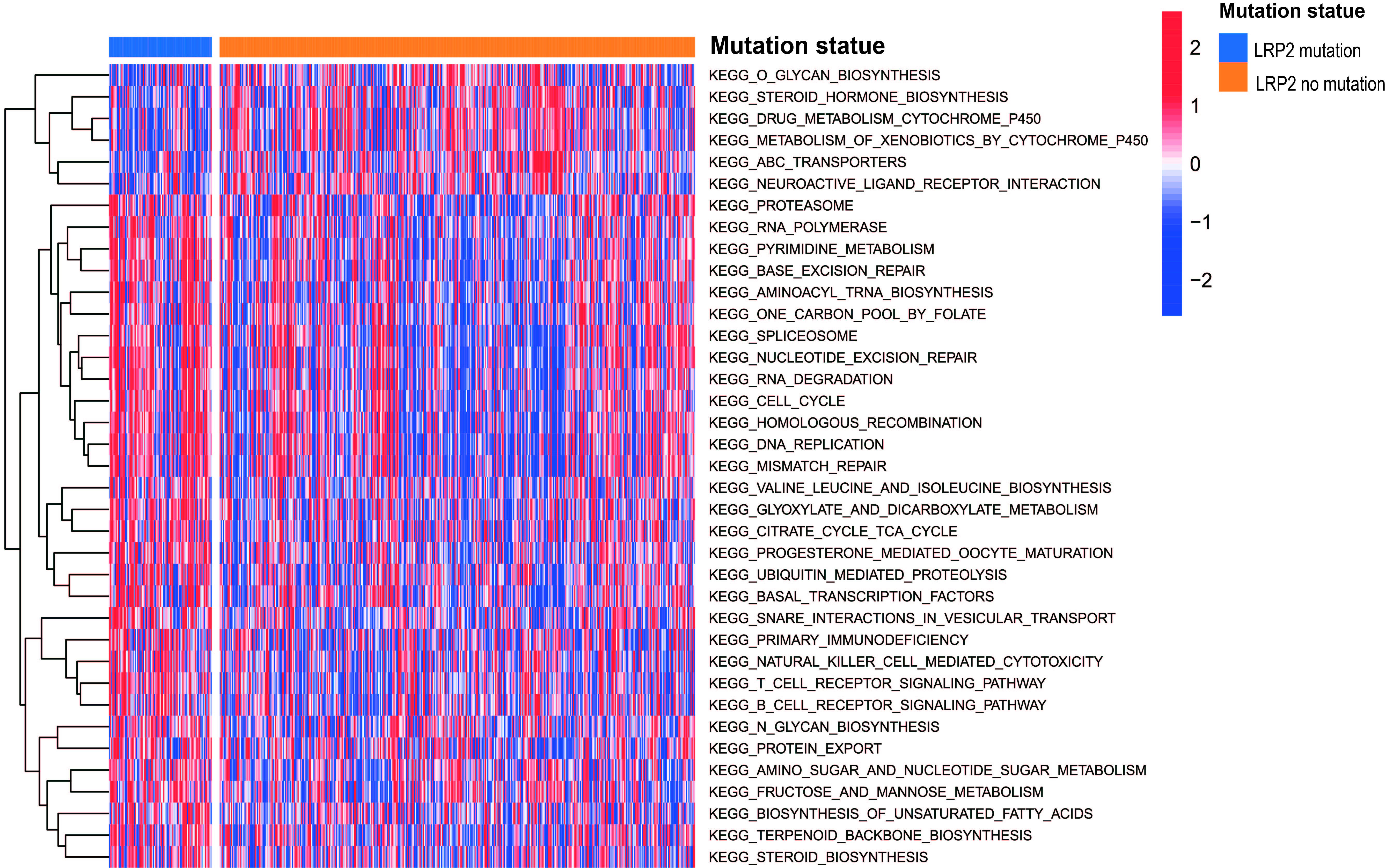
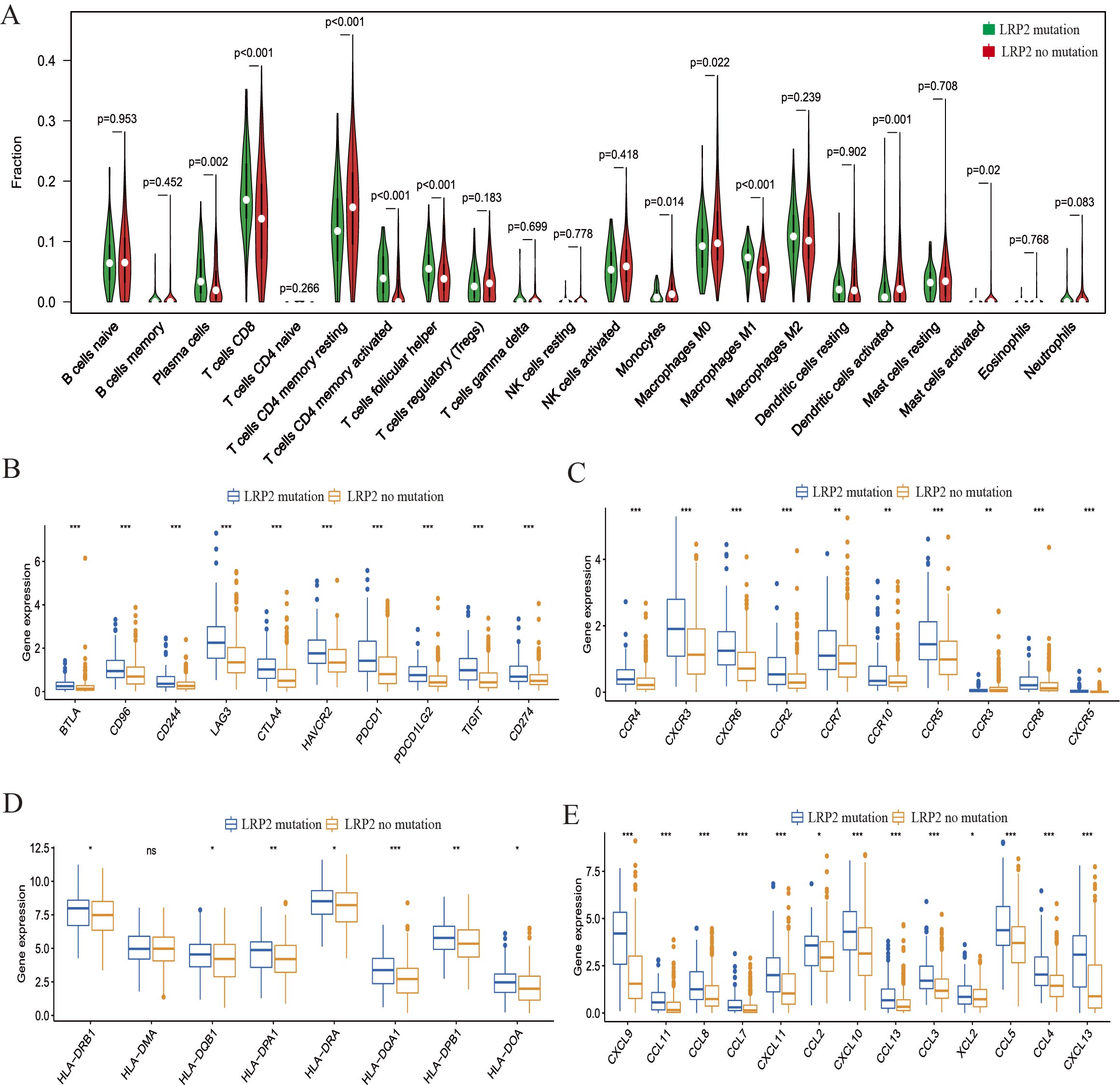
In the TCGA cohort, our results showed that LRP2 mutation was associated with high infiltration level of CD8+ T cells, plasma cells, activated CD4+ memory T cells, and M1 macrophages, but low level of M2 macrophages and resting mast cells (Fig.2A and Fig.S3A). The expression level of PD-L1 in tumor tissues is one of the important biomarkers for patients to choose ICIs treatment [22-23]. In TCGA cohort, we found that LRP2 mutation was associated with high expression level of multiple immune checkpoint genes, such as PDCD1, PDCD1LG2, LAG2, CD274 (PD1) and CTLA4 (Fig.2B and Fig.S3B). Notably, we found that patients with LRP2 mutation had higher enrichment of immune regulatory-related signaling pathways, such as T cell receptor (p=0.00073), B cell recepotor (0.025), NK cell medicated cytotoxicity (0.0024) and toll-like recepotor signaling pathways (0.00062) (Fig.2C). In addtion, other highly enriched signaling pathways in LRP2 mutation were showed in Fig.S4A.
Then, we analyzed immune cell infiltration and immune checkpoint genes expression among different tumor types. The results showed that the coexpression of LRP2 mutation with immune cells, such as CD8 T cells, M1 macrophages, plasma cell, and activated memory CD4 T cells, were highly correlation in several tumor types, especially for BRCA, COAD, LUAD, UCEC and UCS (Fig.2D). Similarly, the coexpression of LRP2 mutation was highly associated with most immune checkpoint genes in BRCA, COAD, UCEC and UCS (Fig.2E). Then, we analyzed the coexpression of LRP2 mutation with immune receptors, immunostimulators, MHC molecules, and chemokines in several tumor types, such as BLCA, COAD, LUAD, LUSC, SKCM, STAD, UCEC, and UCS, because they have high LRP2 mutation percentage (Fig.S4B). The results showed that the expression of most receptors, immunostimulators, MHC molecules and chemokines in COAD, UCEC, UCS and SKCM in patients with LRP2 mutation was higher than those without LRP2 mutation.
Then, we evaluated the relationship of LRP2 mutation with immunotherapy. Through rigorous screening, we identified three studies on melanoma [24-26] and two studies about lung cancer [27-29] that meet the included criteria. After reviewing the literature, we found that only two patients with lung cancer had LRP2 mutation, so these studies were further excluded. Finally, a total of 211 cases of melanoma with LRP2 mutation were applied to evaluate the effect of immunetherapy (Table.S3). The results showed that the application of these ICIs in patients with LRP2 mutation exhibited higher complete response (CR) and partical response (PR) and low percetage of progressive disease (PD) and stable disease (SD) (Fig.2F). Survival analysis showed that LRP2 mutation was associated with significantly improved OS (p=0.0235) (Fig.2G).
2.3 The characteristic of LRP2 mutation in EC
Based on the above results, we knew that LRP2 mutation may be a prognostic and a predictive biomarker for immunotherapy in EC. Two cohort (TCGA and CPTAC) were studied for the relationship of LRP2 mutation with EC molecular subtype. In TCGA-UCEC cohort, we identified 93 patients with LRP2 mutation in 573 patients (18%) (Fig.3A). Survival analysis showed that high LRP2 mutation was associated with better OS (P=0.00644), DSS (p=0.0141) and PFS (p=0.00483) (Fig.3B), indicating that LPR2 mutation may be a prognostic factor of EC.Then, our results showed that LRP2 mutation was related to high TMB level, MSI MANTIS score and MSIsensor Score (Fig.3C). Then, we compared the mRNA difference between LRP2 mutation and LRP2 no mutation in EC. The results showed that LRP2 mutation was related to the high expression level of CXCL9, TIGIT, CXCR6, CXCL13. ICOS and LAG3, all of which were involved in immune regulation (Fig.3D). GO and KEGG analysis confired the high enrichment level of immune related signaling pathways, such as T cell activation/differentiation, chemokine-medicated signaling pathway, response to chemokine, lymphocyte migration and chemokine signaling pathway (Fig.3E-F). Other highly enriched signaling pathways included DNA replication, cell cycle, homologous recombination, mismatch repair, NK cell-mediated cytotoxicity, N-glycan biosynthesis and TCA cycle (Fig.S5). Similar with the outcomes from pan-cancer analysis, the LRP2 mutation in TCGA-UCEC also presented higher infiltration CD8 T cell, plasma cells, and M1 macrophages than that without LRP2 mutation (Fig.S6A). In addition, our outcomes showed that the expression of most immune receptors, immunostimulators, MHC molecules and chemokines in patients with LRP2 mutation was higher than those without LRP2 mutation in TCGA cohort (Fig.S6B-E).
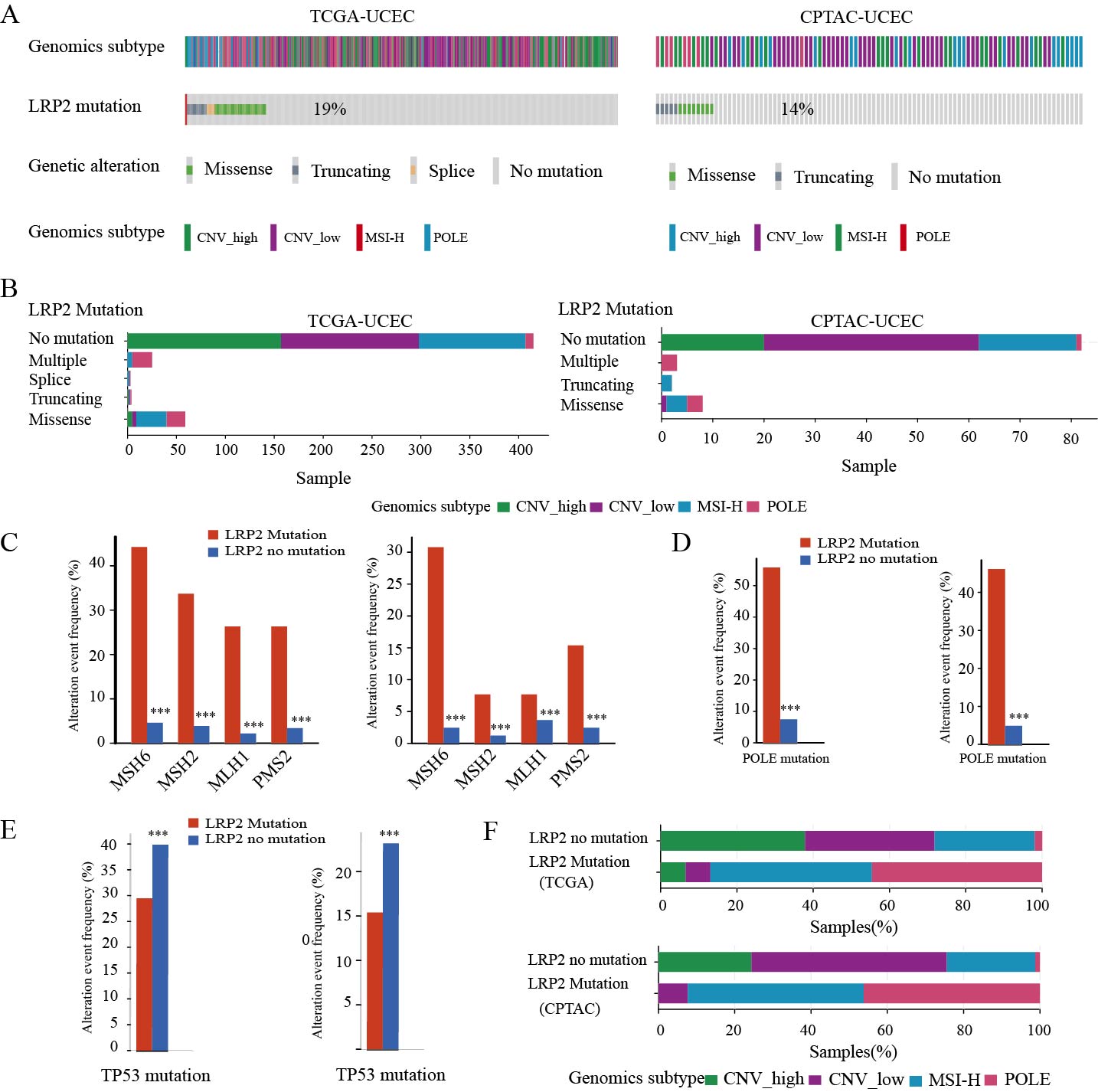
The Cancer Genome Atlas (TCGA) performed a genome-wide analysis of 373 EC and identified four distinct groups: CNV-high, CNV-low, MSI-H, and POLE type [30]. POLE tumors were more common in earlier stages and the prognosis for these patients was excellent. MMRd tumor (MSI-H) had high mutation frequency, potential imunotherapeutic response and good prognosis. The CNA-low (also defined as p53 wt) subgroup was found to be quite heterogeneous and exhibited different prognosis since it covered multiple pathologic types of tumors. However, in CNA-high subgroup (also defined as p53 alterations) with p53 either overexpression or missense are associated with the worst prognosis of all molecular subtypes. The tumor subgroup includes most serous and mixed types, which occur at a higher stage, usually grade 3 [31]. In both cohorts, we evaluated the association between LRP2 mutation and four molecular subtypes in EC. In TCGA cohor, we identified 95 patients with LRP2 mutation in 509 patients (19%) (Fig.S7A) and missense mutation was the main type of mutation (Fig.S7B). In CPTAC cohort, we identified 13 patients with LRP2 mutation in 95 patients (14%) (Fig.S7A), with missense mutaitons being the main mutation type (Fig.S7B). Compared with patients without LRP2 mutation, patients with LRP2 mutation harbored more MMR mutant genes in TCGA and CPTAC cohort, indicating that patients with LRP2 mutation had high MSI levels (Fig.S7C). Then, we compared the association of LRP2 mutation with POLE and TP53 mutation in both cohorts. Our results showed that most patients with LRP2 mutation had higher percentage of POLE mutation and lower TP53 mutation than those without LRP2 mutation (p<0.001) (Fig.S7D-E).
Finally, we compared the association of patients with LRP2 mutation with EC molecular types. Our results showed that in TCGA cohort, 41 patients (43.16%) with LRP2 mutation belonged to POLE type and 39 patients (41.05%) with LRP2 mutation belonged to MSI-H type, but only 14 patients were CNV-low or CNV-high type (14.74%) (Fig.S7F). In CPTAC cohort, 6 patients with LRP2 mutation corresponded to POLE type, 6 patients were MSI-H type and only 1 patients belonged to CNV-low type (Fig.S7F). These outcomes indicated that LRP2 mutation can help to exclude highly malignant tumors and select tumors with high response of immunotherapy.
2.4 Development and validation of a prognostically useful LRP2 mutant signature
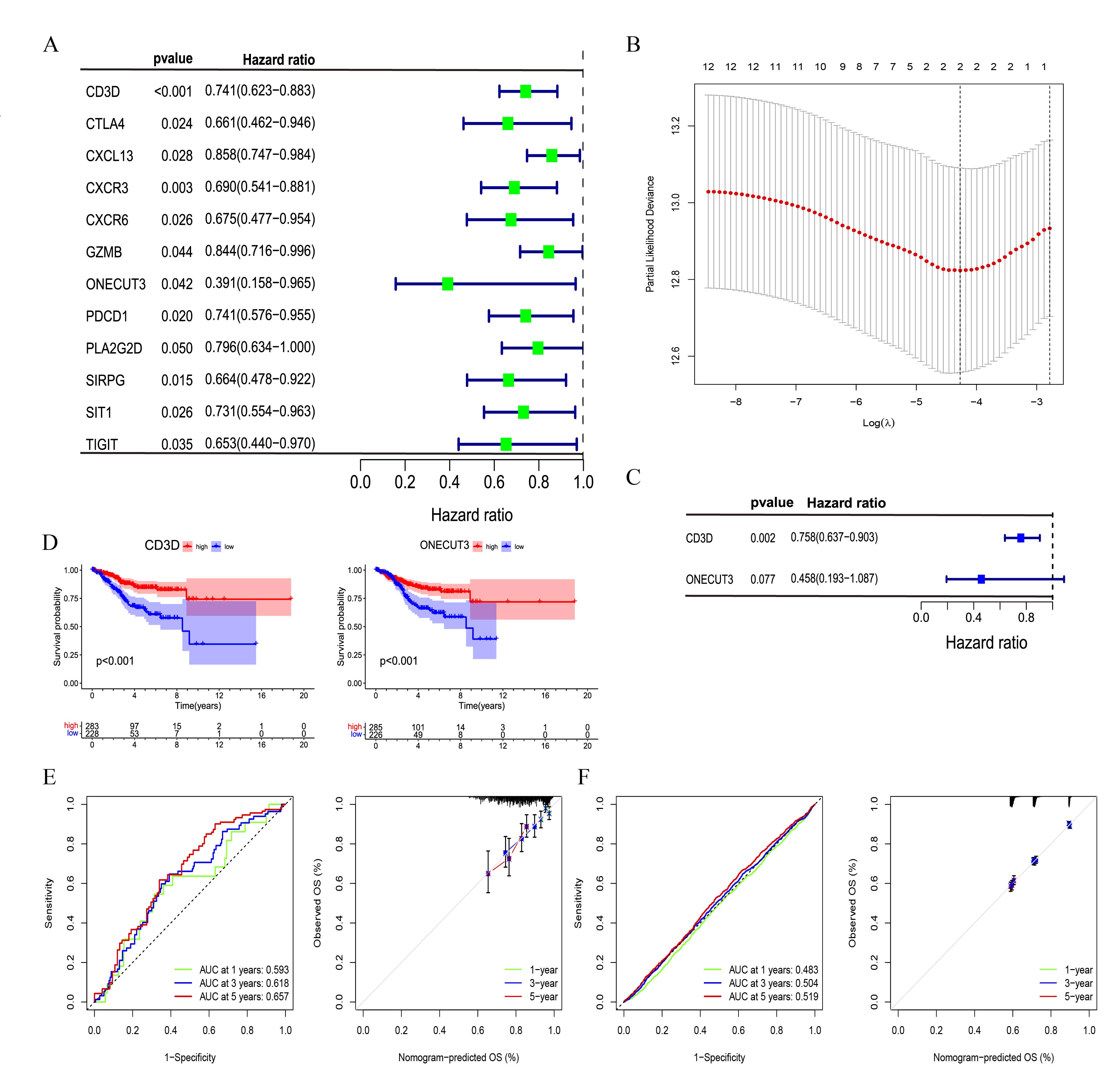
There are numerous studies examining whether genetic mutation affects the efficacy of immunotherapy and patients survival [32]. In this study, we found that LRP2 mutation were not statistically association with prognosis in most TCGA cancer types. Notably, LRP2 mutation in UCEC was significangly associated with OS, DSS and PFS (Table.S2). Using LRP2 mutation as a prognostic marker, while useful in some contexts, may not be useful in others. For example, LPR2 mRNA level and protein function can be inactivated by LRP2 mutation. In this study, we found no significant differences between LRP2-mutated and non-LRP2-mutated in the EC and pan-cancer cohort (Fig.4A). Thus, we sought to develop an RNA expression signature correlated with LRP2 mutation that might be more prognostic. We tested a mutant LRP2 expression signature based on the expression of genes consistently upregulated in mutant LRP2 EC patients (Table.S4). Then, unitrivariate regression analysis was undertaken to identify key prognostic markers in EC cohort (Fig.S8A). LASSO Cox analysis were performed (Fig.S8B) and two genes (CD3D and ONECUT3) were finally selected to establish a prognostic signature (Fig.S8C). The formula was shown as: LMS score =0.276627*expression level of CD3D+0.780825*expression level of ONECUT3. The two genes were risky prognostic genes (Fig.S8D). All patients were divided into high LMS and low LMS groups based on the optimal LMS score=0.585, that was founded by “Cutoff Finder”. Then, we compared the effect of LMS score in predicating prognosis with LRP2 mutation status and showed that LMS had higher accuracy with narrow confidence intervals than LRP2 mutation (Fig.4B). In EC and pan-cancer data, LRP2 muation exhibited higher LMS score than those without LRP2 mutation (Fig.4C). Survival analysis showed that patients with high LMS score had longer overall survival compared with the low LMS group in the EC (Fig.5D) and pan-cancer cohort (Fig.5E). The area under the ROC curve and calibration plot was used for predicting 1-year 3-year and 5-year OS (Fig.S8E-F). Finally, we applied the Web-based software program Kaplan-Meier Plotter on 11 TCGA cancer types using these two gene signature and found a strong correlations between our prognostic calculations and the Kaplan-Meier Plotter-based calculations (Table.S5). Meanwhile, we demonstrated the association of LMS score with LRP2 mutational signature, survival status and gene expression in EC (Fig.4F) and pan-cancer cohort (Fig.4G).
2.5 Relationship of LMS score with TMB, MSI and immune microenvironment
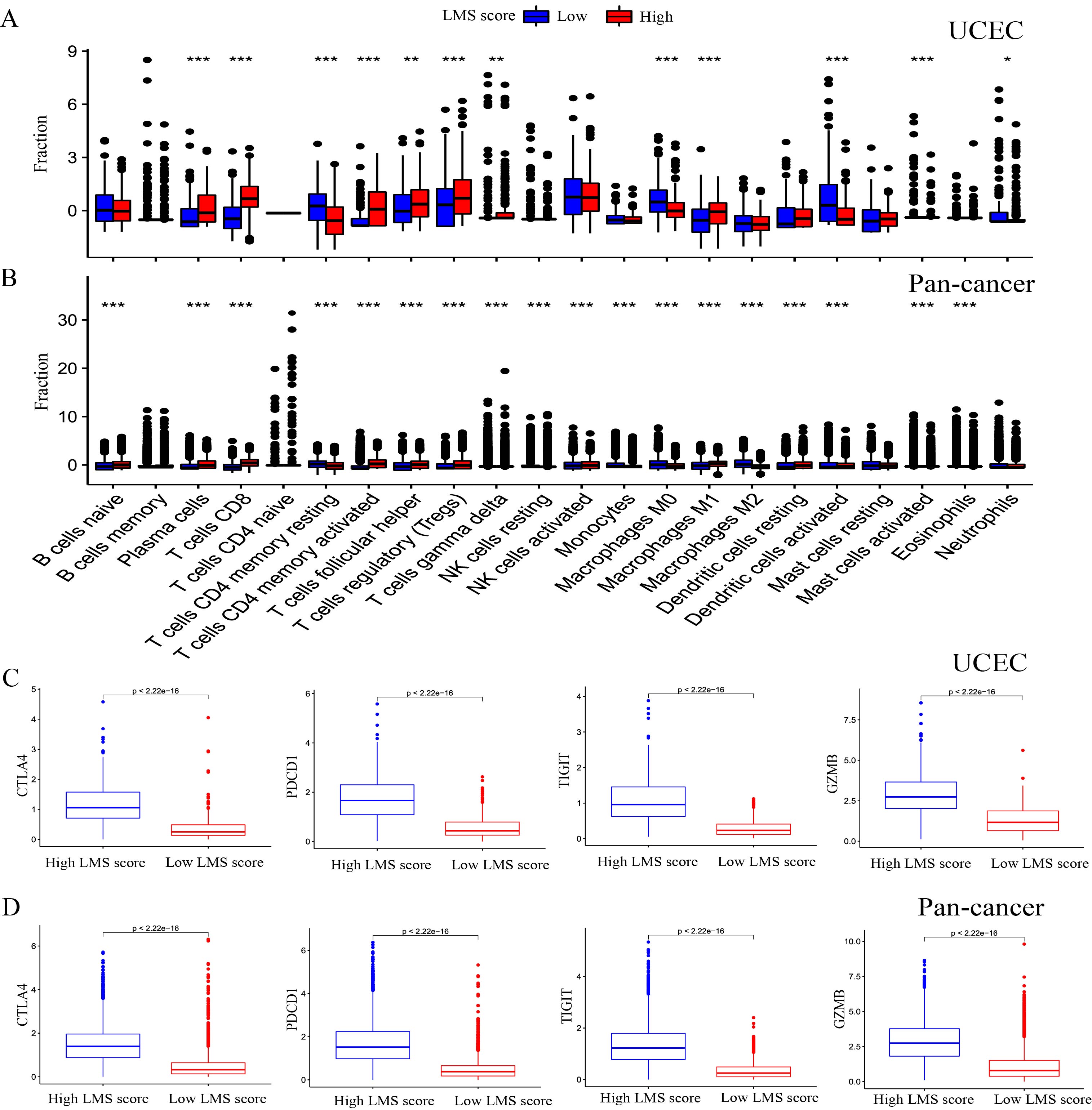
To further evaluate the potential of LMS score as a predicator of immunotherapy, we explored the relationship of LMS to TMB, MSI and the immune microenvironment. Our study unvealed a positive correlation between LMS score and mutation count, MSI sensor score and MSI MANTIS score in EC (Fig.5A) and pan-cancer cohort (Fig.5B). Importantly, further analysis revealed that LMS score was significantly and positively associated with TMB in several cancer types, including UCEC, THYM, THCA, TGCT, LGG, and COAD (Fig.5C). Likewise, there was a significant association of LMS with MSI in UCEC, TGCT, OV, LUSC, and COAD (Fig.5D). To better understand the association of LMS with the immune-infiltratiing microenvironment, we investigated the composition of 22 types of immune cells between high LMS and low LMS group in EC and pan-cancer cohort. Compared with the low LMS group, high LMS was signaficantly associated with higher infiltration of CD8 T cell, activated CD4 T cell, M1 macrophage, and plasma, while exhibited low infiltration of M0 macrophage, resting memory CD4 T cell and activated dendritic cells (Fig.SA-B). At the same time, we also analyzed the relationships between immune checkpoint expression and LMS. Our results revealed that high LMS was significantly and positively associated with expression of important immune checkpoints expression, including CTLA4, PDCD1, TIGIT and GZMB in EC (Fig.S9C) and pan-cancer cohorts (Fig.S9D).
Recently, a new global transcriptomic immune classification of solid tumours has identified six immune subtypes (ISs) (C1-C6): wound healing (C1), IFN-g dominant (C2), inflammatory (C3), lymphocyte depleted (C4), immunologically quiet (C5) and TGF-b dominant (C6). Of the C1-C6 subtypes, C4 and C6 subtypes conferred the worst prognosis on their constituent tumors and displayed composite signatures reflecting a macrophage dominated, low lymphocytic infiltrate, with high M2 macrophage content. In contrast, C2 and C3, have the favorable prognosis [33]. In this study, we found that the high LMS group had a high percentage of C2 and C3 subtypes and a low percentage of C1 and C4 subytpes compared to those in low LMS group (Fig.5E). Similarly, in the pan-cancer analysis, nearly half of patients in high-LMS group were C2 subtype, but the percentage of the C4 subtype was lower than those in low LMS group (Fig.5F).
2.6 LRP2 mutation signature predicating the efficacy of immunotherpy
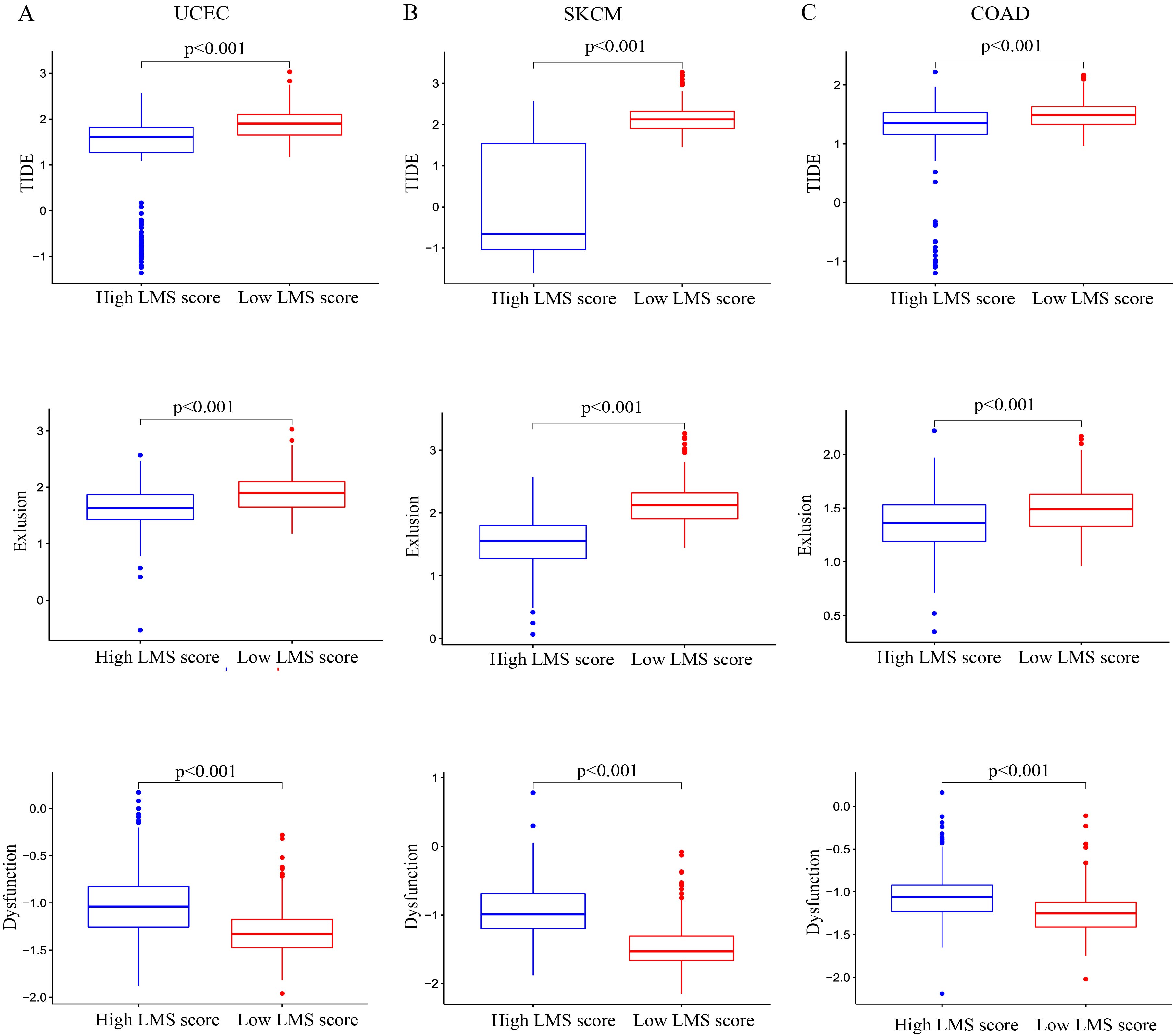
To infer the potential role of LMS in prdicating immunotherapy efficacy, we calculated IPS in pan-cancer patients. The results indicated that high LMS was assocaited with higher IPS compared to low LMS score (Fig.6A). Then, we compared the difference of TIDE between high LMS group and low LMS group in UCEC, SKCM, and COAD. The results showed that patients in high LMS group had higher immune dysfunction, and low TIDE and immune exclusion level than those in low LMS group (Fig.S10A-C), suggesting the potential better responses to immuotherapy.
Finally, to validate the predictive power of LMS in immunotherapy, we analyzed the all experimental studies on immunotherapy on the TIDE platform. According to the inclusion criteria, a total of 8 studies with 307 patietns was included for further analysis (Table.S5). Then, we performed a meta-analysis, and the results showed that patients in high LMS group had higher response rate than those in low LMS group (OR 1.55. 95% CI 1.16-2.08, p=0.003) (Fig.6B). The funnel plot confirmed the reliability of the results (Fig.6C). Then, we included two studies to evaluate the association of LMS with clinical resposne to immunotherapy and prognosis. In the cohort of Gide et al, a high LMS score was associated with a better clinical response to immunotherapy (chi-square test, p<0.001) (Fig.6D). Survival analysis exhibited that patients with high LMS score had better prognosis than those with low LMS score (log-rank test, p=0.044) (Fig.6E). In the IMvigor210 cohort, the proportion of responders (CR/PR) was higher in the high LMS group than in low LMS score group (chi-square test, p < 0.05) (Fig.6F). Survival analysis also confimred that patients with high LMS score had better prognosis than those with low LMS score (log-rank test, p=0.030) (Fig.6G). The ROC curve demonstrated that the survival AUC were 0.895, and 0.584 in Gide and IMvigor210 cohort, respectively, indicating a high accuracy of the model (Fig.6H).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}