A model’s overall performance can be interpreted from its LHR + and AUC values (25–27). For patients in the high risk group, the scoring model’s LHR + was 3.47 (95% CI: 2.60, 4.64). For an LHR + of 2 to 5, use of the model could presumably influence the pre-test to post-test probability (27). With a pre-test probability of 59.9% (CBD stone prevalence in this study), the CBD stone probability (i.e., post-test probability or positive predictive value) shifted to 83.9%, approximately 20% higher than the pre-test value. For the low-intermediate risk classification, the LHR + was 0.16 (95% CI: 0.09, 0.27). For an LHR + between 0.1 and 0.2, the model had a moderate likelihood of influencing pre-test to post-test probability (27). The probability of stone absence increased from 40.1–81.0% (i.e., negative predictive value); the probability of CBD stone presence decreased from 59.9–19.0%. The AUC value reflects a model’s overall performance. The scoring model had an AUC of approximately 0.80 (95% CI: 0.76, 0.83); its discrimination properties were acceptable to excellent (AUC 0.70–0.80) (26). The internally validated AUC slightly decreased but remained near 0.80 (0.76; 95% CI: 0.72, 0.81). The proposed model exhibited significantly better performance than did the ASGE and ESGE guidelines for CBD stone prediction in the high-prevalence population, according to the comparative validation (AUC and decision curve analysis) (Fig. 5).
Concerning model predictors, we found that pancreatitis was a negative predictor, while cholangitis did not reach statistical significance. Regarding the negative for score pancreatitis, our results are consistent with published findings that most CBD stones in pancreatitis patients often spontaneously pass into the gastrointestinal tract (28); a less-invasive investigational approach is appropriate in such patients (17). Furthermore, cholangitis, a strong clinical predictor of CBD stones (5, 10), was a non-significant variable in our multivariable analysis. This outcome is also consistent with previous literature (29, 30). The use of cholangitis as a sole predictor could be an important reason for the limited predictive ability of current guidelines. Notably, ALP was a potent predictor. ALP level > 250 mg/dL had the highest odds ratio (3.35; 95% CI: 2.02, 5.55). The significance of the ALP and CBD stone relationship has been extensively analyzed (3, 31, 32). However, ALP has minimal importance in current guidelines. Our findings suggest that more attention to ALP may be useful in future guidelines or the construction of predictive models.
Our scoring system is based on assessment of patient-specific predictors. The sum of assigned predictor scores (Table 2) serves as the individual patient’s model-based score. The individual patient’s score is used to support the assessment of CBD stone probability, together with the risk group classification. According to risk curve analysis, a higher score was associated with a higher probability of CBD stone presence (Fig. 4). Our scoring model can also be used in s/p cholecystectomy and cirrhotic patients, although these factors can affect CBD size and LFT results (23, 24).
When implementing the model, additional factors should be considered with respect to the availability of expert physicians and specialized equipment. Although the model could reasonably reduce the probability of CBD stones for the low-intermediate risk group, the probability remained moderate (i.e., 20–30%). IOC (or laparoscopic ultrasound (33)) may be the most reasonable approach because cholecystectomy can be performed in the same setting (34). However, for physicians or hospitals without the capability to treat detected stones, there may be a need for patient transfer or the use of less-invasive investigations (e.g., MRCP or endoscopic ultrasonography) (35). Laparoscopic bile duct exploration (trans-cystic/trans-ductal) (36) or same-setting ERC (i.e., ERC combined with cholecystectomy) (7) are potential methods for removal of IOC-detected CBD stones. However, because patients with CBD dilatation only comprised 12.9% (n = 11) of our cohort, trans-ductal CBD exploration could not be applied because it requires a dilated duct (36). In the absence of alternative interventions for IOC-detected CBD stones, possible treatment options are trans-cystic biliary stent insertion followed by transfer for ERC (in an ERC-capable hospital) (37), or the acquisition of a clear cystic duct (e.g., via ligation or clipping of the cystic duct stump to prevent leakage related to high pressure from the retained CBD stone) followed by rapid transfer. Postoperative abdominal pain or cholangitis can occur in patients with persistent stones (38). Persistent CBD stones are unlikely to increase the probability of cystic duct stump leakage, although they can aggravate its severity (39).
Our proposed model sufficiently increased the CBD stone probability that is appropriate for consideration of ERC in the high risk group (i.e., from 59.9–83.9%). However, our short survey indicated that some physicians expect near 100% CBD stone probability; endoscopic ultrasonography and ERC in the same setting may be optimal (40). This approach can almost avoid the need for diagnostic (unnecessary) ERC. However, because most CBD stone patients are older adults, the prolonged procedural time, increased sedation (41), and cost can limit the application of combined endoscopic ultrasonography and ERC. The scoring model may improve patient selection for this combined approach.
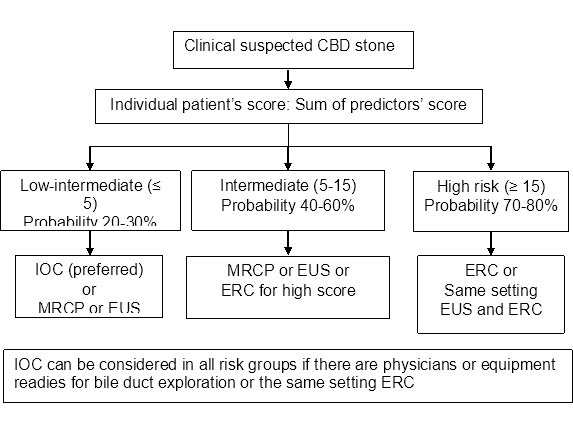
The intermediate-risk group might constitute an indeterminate group. The CBD stone chance was moderate (49.8% in our cohort); a less invasive investigation (e.g., MRCP or endoscopic ultrasonography) may thus be more suitable. Nevertheless, IOC is appropriate for all risk groups if experienced surgeons and specialized equipment are available (42). In the Supplemental Figure, we show a proposed CBD stone investigation and treatment flow approach regarding specific risk groups; we provide example checklists for clinical application in Supplemental Table 2.
There were considerable limitations in our study. First, we reviewed data from reference tests. Some patients with suspected CBD stones were not included in our data; other patients had few unusual findings in LFTs or imaging result abnormalities, and attending physicians chose observation as management for such patients. Thus, there were no reference test records for these patients. However, we considered the outcome validity to be an essential focus of the study; we did not modify the study protocol. With a similar potential selection bias issue, our reference tests were not included all CBD stone confirmatory tests. Endoscopic ultrasonography was not available in the study hospital during the study period. Second, a retrospective design is not the optimal data collection approach for a model development study because it involves various potential biases (15). Third, for the proposed application, LFTs should be examined within 7 days before using the score-based model to assess the CBD stone risk or choose a reference test that is compatible with our study protocol. Finally, the CBD prediction model was developed using data from patients with relevant clinical manifestations and a high-prevalence population. Thus, the findings cannot be applied to a low-prevalence population until they have been confirmed in additional studies.
{kind=link}