Design, settings and participants
The Japan COVID-19 and Society Internet Survey (JACSIS) undertook an epidemiological approach to investigate the social and individual health situations related to the COVID-19 pandemic. In JACSIS, 28,000 respondents were investigated from among 224,389 qualified panelists selected through approximately 2.2 million panelists registered with a Japanese Internet survey agency (Rakuten Insight, Inc., Tokyo, Japan). The participants were recruited using a random sampling method to select a sample representative of the official demographic composition of Japan as of October 1, 2019, based on the categories of age, sex, and region of residence (i.e., all 47 prefectures). A cross-sectional design was used to detect changes in individual lifestyle and social factors before and after the COVID-19 pandemic. Web-based informed consent was obtained from all participants before they completed the online questionnaire.
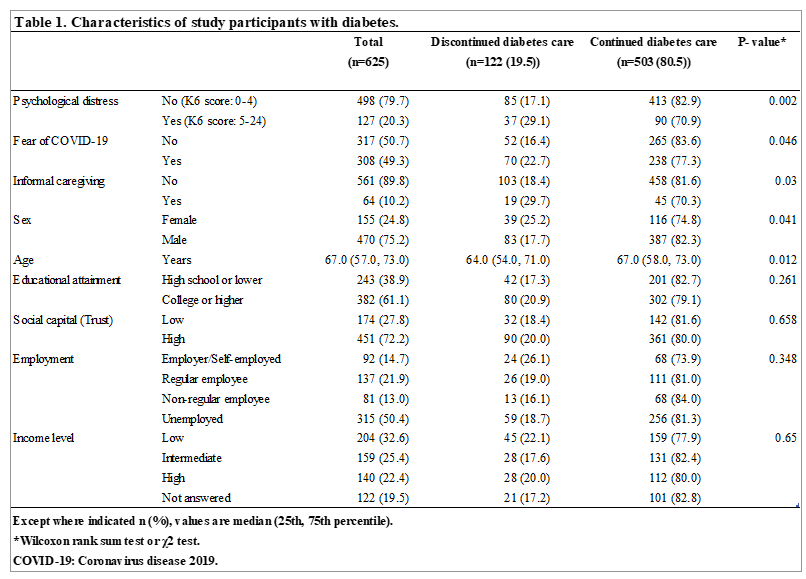
Of the 28,000 respondents, 625 patients with diabetes (155 women and 470 men) were analyzed (Table 1). First, we excluded 2,518 participants who provided invalid responses. These measures to validate the quality of the data consistently were performed as described in previous studies [17-20]. Second, we excluded 23,917 participants without comorbid diabetes. Finally, we excluded participants who had not visited the hospital (n = 449) or had comorbidities (n = 490). In this survey, asthma, bronchitis, pneumonia, atopic dermatitis, otitis media, angina pectoris, myocardial infarction, stroke, chronic obstructive pulmonary disease, cancer, malignant tumors, chronic pain, depression, and mental disease (without depression) were defined as comorbidities.
The protocol for this research conforms to the provisions of the Declaration of Helsinki. This study was reviewed and approved by the Research Ethics Committee of the Osaka International Cancer Institute (No. 20084). In this study, the data used are not deposited in a public repository, due to confidentiality and restrictions being imposed by of data the Research Ethics Committee of the Osaka International Cancer Institute. Data inquiries should be addressed by data manager (Takahiro Tabuchi: [email protected]).
Measurements
The outcome variable was “refraining from visiting the hospital as scheduled between April and May 2020” by patients with diabetes. The outcome was obtained from a specific question: “Did you refrain from a planned hospital visit between April and May 2020?” The answer options were “yes”, “no”, and “not applicable (not planning on visiting the hospital)”. Patients with diabetes who answered “not applicable” were excluded from the analysis.
The main exposure variables were fear of COVID-19 and psychological distress. We used the Fear of COVID-19 scale (FCV-19S) to assess anxiety and fear of COVID-19. The FCV-19S has been validated in recent Japanese studies [6, 21, 22]. The FCV-19S is composed of seven statements, and the total score is calculated by adding up each item score (range = 7–35). The higher the score, the greater the fear of COVID-19. Total scores of 19–35 were defined as having a fear of COVID-19 (the cutoff score was defined as the median of patients with diabetes in this study). We used the 6-item Kessler Screening Scale for Psychological Distress (K6) to measure psychological distress. The total score on the K6 ranges from 0–24. We used a proven reliable and validated Japanese version of the K6 in this survey [23]. A K6 score ³5 was used to indicate the presence of mild psychological distress [24].
In a path analysis, psychological distress was considered a mediator of fear of COVID-19 to refrained diabetes care, as described below. In a previous study, COVID-19 pandemic-associated anxiety and fear were found to be positively correlated with perceptions of vulnerability to infection [25]. We adjusted for SES as follows: informal caregiving (categorized as “yes [providing care primarily] or yes [providing care, but not primarily]” or “no [not providing]”), educational attainment (categorized as “high school or lower” or “college or higher”) [26], employment (“employer”, “self-employed”, “regular employee”, “non-regular employee”, and “unemployed”) [27], trust in neighbors (categorized as “high [trust or moderately trust]” or “low [not trust or moderately not trust]”) [28], and income level (categorized by tertiles of household equivalent income in 2019 [low, <4 million JPY; intermediate, 4–7 million JPY; high, >7 million JPY; unknown or no answer]) [29].
Statistical analyses
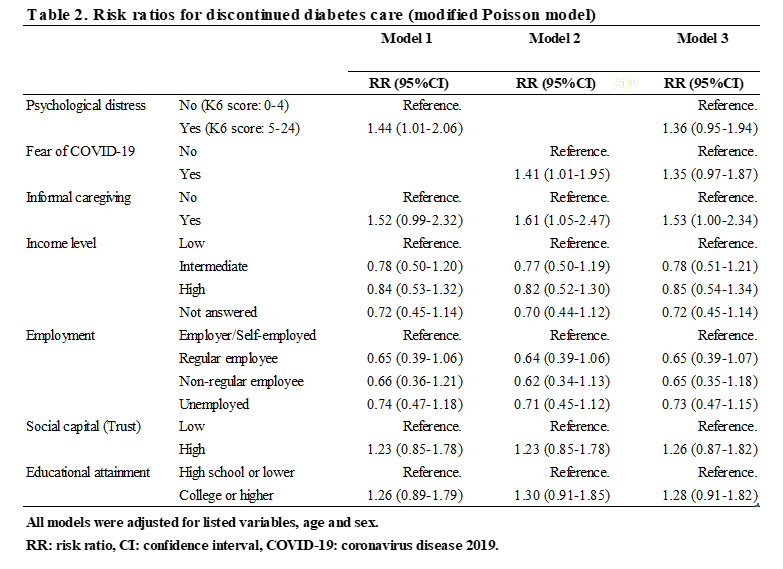
A modified Poisson model was applied to calculate risk ratios (RRs) for the association between diabetes care and mental condition (fear of COVID-19 and psychological distress) during the COVID-19 pandemic (Table 2). We designed three models to assess the effects of psychological distress and a fear of COVID-19 on diabetes care. Model 1 included only psychological distress, model 2 included a fear of COVID-19, and model 3 included both psychological distress and a fear of COVID-19. All models were adjusted for age, sex, informal caregiving, income level, employment, trust in neighbors, and educational attainment.
To examine the statistical mediation effects, a path analysis using structural equation modeling (SEM) was performed. The SEM tested the direct effects from a fear of COVID-19 to continued diabetes care, and the indirect effects from a fear of COVID-19 to continued diabetes care via psychological distress. A fear of COVID-19 and psychological distress were modeled as continuous variables. Informal caregiving, employment, and trust in neighbors were included in the SEM as endogeneity of both fear of COVID-19 and psychological distress. Unstandardized profit regression coefficients with 95% confidence intervals (CIs) are reported with a root mean square error of approximation (RMSEA) ≤ 0.08 [30]. Good model fit was indicated by both a goodness-of-fit index (GFI) ³ 0.90 and an adjusted goodness-of-fit index (AGFI) ³ 0.90.
All statistical analyses were performed using STATA 12.0 (Stata Corp, College Station, TX, USA) and JMP ver. 16.1 (SAS Institute Inc. Cary, NC, USA). This study followed the STROBE guidelines for a cross-sectional study.
{kind=link}
{kind=link}