Study Cohort
The project recruited 521 consecutive patients who underwent elective primary THA or TKA at Fairfield Hospital, Sydney between August 2018 and May 2019. Out of 521 patients recruited, 500 were included in our study. Of the 21 patients excluded, 19 had imaging and pathology records that were either incomplete or inaccessible to our investigators, one patient died intra-operatively, and one patient had two admissions during the study period, of which the second admission was excluded.
Characteristics of the study population
The mean age of our cohort was 67.9 years (SD: 9.6) and 329 (65.8%) were female. Three hundred and sixty-nine patients (73.8%) received a TKA, whereas 131 (26.2%) received a THA. Most patients (405; 81.0%) experienced no complications during their acute hospital stay; 73 (14.6%) experienced only minor complications and 22 (4.4%) experienced at least one major complication. Of the 22 who experienced a major complication, 6 (27.3%) also experienced minor complications. The three groups were similar at baseline, though a greater proportion of people with complications also had cardiovascular disease (p=0.04), hypertension (p=0.04) and renal impairment (p=0.04). The median length of stay was 4.0 days (range: 1.0–13.0) in patients with no complications, 6.0 days (range: 2.0–21.0) in those who experienced minor complications and 5.0 days (range: 2.0–14.0) in those with major complications (p<0.001). The rate of admission to an intensive care unit or high-dependency unit (ICU/HDU) was 3.2% in patients with no complications, 9.6% in patients with minor complications, and 18.2% in those with major complications (p<0.001; Table 1).
Complications
We recorded 116 complications in 95 people, 94 of which were minor complications, and 22 of which were major complications. A greater proportion of patients undergoing THA experienced major complications compared to those undergoing TKA (11 out of 131 [8.4%] of THA patients versus 11 out of 369 [3.0%] of TKA patients; p=0.025) (Additional File 4). Joint-related complications affected 50 (10.0%) patients during their stay. The most common joint-related complication was minor wound bleeding or oozing requiring vacuum dressing, which affected 37 (7.4%) patients. Other types of joint-related complications were rare, such as fracture (n=4; 0.8%), major bleeding (n=3; 0.6%) and superficial surgical site infection (n=3; 0.6%). On the other hand, non-joint related complications affected 56 (11.2%) patients during their stay. The most common minor non-joint-related complications was cardiac arrhythmia (n=11; 2.2%), followed by delirium (n=10; 2.0%), urinary tract infection (n=8; 1.6%) and electrolyte disturbance (n=7; 1.4%), and the most common major non-joint-related complication was a respiratory complication (n=7; 1.4%). No venous thromboembolisms were diagnosed during the acute care period in this cohort though several patients were investigated for this outcome. For all complications recorded see Additional File 4.
Cost of Investigations
Imaging and pathology cost per patient by complication status
Complication status was associated with both the total number and total cost of imaging and pathology tests per patient. The mean number of imaging tests was 1.5 (SD: 0.7) in patients with no complications, 2.4 (SD: 1.6) in patients with only minor complications and 3.5 (SD: 2.3) in those with at least one major complication (p<0.001). The mean number of pathology tests was 5.5 (SD: 4.3) in patients with no complications, 13.5 (SD: 14.9) in patients with only minor complications and 18.3 (SD: 18.0) in those with at least one major complication (p<0.001). In an adjusted negative binomial model, we found that patients with only minor complications received more imaging tests (aIRR: 1.49; 95% CI:1.24–1.78) and more than double the number of pathology tests (aIRR: 2.07; 95% CI:1.74–2.47) relative to those with no complications. Patients with at least one major complication received more than double the number of imaging (aIRR: 2.07; 95% CI:1.59–2.65) and triple the number of pathology tests (aIRR: 3.00; 95% CI:2.26–4.04) compared to patients with no complications.
As the number of tests increased with each level of complication status, the mean total cost increased concomitantly. In patients with no complications, the total imaging costs were AU$ 88.9 (SD: 101.8) and pathology costs were AU$ 97.7 (SD: 83.6) per patient (Table 2; Figure 1 & 2). In an adjusted linear regression model, patients with only minor complications incurred more than double the cost compared with patients with no complications, with mean additional costs per patient of AU$ 103.7 (95% CI: 66.2–141.1) for imaging and AU$ 136.3 (95% CI: 98.0–174.5) for pathology. Among patients with at least one major complication, the costs for imaging and pathology tests were more than three times higher than for those with no complications, with mean additional costs per patient of AU$ 231.4 (95% CI: 167.4–295.5) for imaging and AU$ 217.2 (95% CI: 151.8–282.6) for pathology.
Regardless of complication status, every ICU/HDU admission prompts a series of pathology screening tests used to detect multi-drug resistant microorganisms. The mean number of pathology tests in those admitted to ICU/HDU was 26.2 (SD: 18.0), compared to 6.3 (SD: 6.6) in those who were not admitted to ICU/HDU (p<0.001).
Table 2. Mean cost (in AU$) of imaging and pathology tests performed per patient, with additional cost by complication status in AU$.
|
|
No complications
N = 405
|
Minor only
N = 73
|
Major, at least one
N = 22
|
|
Imaging
|
|
|
|
|
Mean cost (SD)
|
88.9 (101.8)
|
201.7 (251.3)
|
337.4 (299.4)
|
|
Additional costa, unadjusted (95% CI)
|
Reference
|
+ 112.8 (76.3–149.4)
|
+ 248.5 (185.7–311.4)
|
|
Additional cost, adjustedb (95% CI)
|
Reference
|
+ 103.7 (66.2–141.1)
|
+ 231.4 (167.4–295.5)
|
|
Pathology
|
|
|
|
|
Mean cost (SD)
|
97.7 (83.6)
|
250.3 (285.5)
|
329.0 (323.8)
|
|
Additional costa, unadjusted (95% CI)
|
Reference
|
+ 152.7 (115.7–189.6)
|
+ 231.3 (167.6–295.0)
|
|
Additional cost, adjustedb 95% CI)
|
Reference
|
+ 136.3 (98.0–174.5)
|
+ 217.2 (151.8–282.6)
|
a Additional cost represents the cost that is added when the specified type of complication is present, compared to when it is absent.
b Adjusted for age, sex, procedure, ASA score, operation time (minutes), anxiety and depression, cancer (past and current), diabetes mellitus, dementia, hypertension, hyperlipidaemia, hyperthyroidism, osteoporosis, urinary incontinence, chronic urinary tract infection, and autoimmune, cardiac, chronic respiratory, cerebrovascular, central nervous system, liver, renal, gastro-oesophageal reflux disease, and past venous thromboembolism.
Figure 1. Mean cost of imaging tests performed per patient, by complication status.
Figure 2. Mean cost of pathology tests performed per patient, by complication status.
Imaging and pathology tests by overall cost contribution
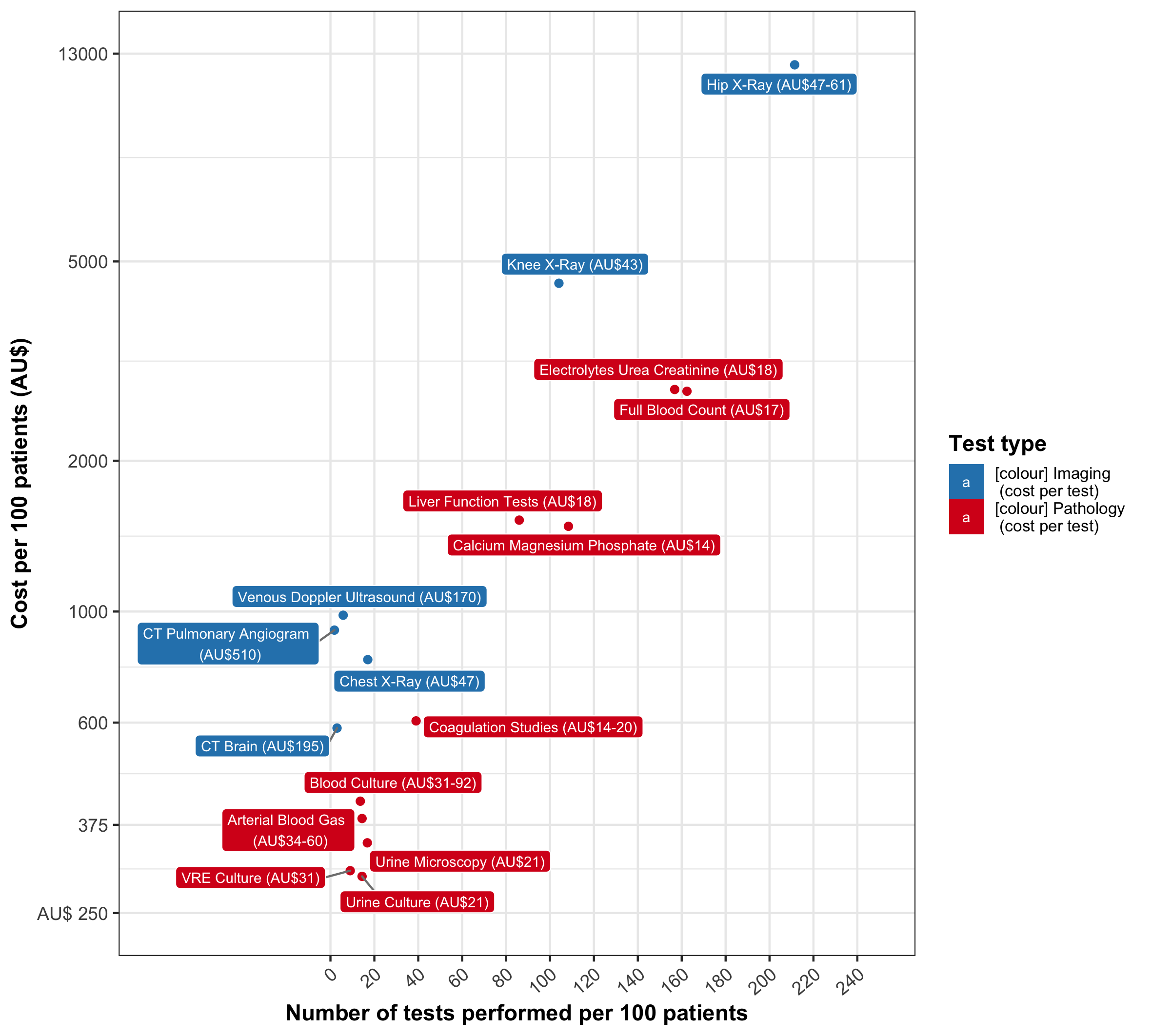
The imaging tests contributing most to the overall cost burden of this cohort were: hip x-ray (mean AU$ 121.0 per THA patient; SD = 31.1; n = 277), knee x-ray (mean AU$45.2 per TKA patient; SD = 9.5; n = 384), venous doppler ultrasound (mean AU$ 9.8 per patient; SD = 41.1; n = 29), CT pulmonary angiogram (mean AU$ 9.2 per patient; SD = 67.9; n = 9), chest x-ray (mean AU$ 8.0 per patient; SD = 24.3; n = 85) and CT brain (mean AU$ 5.9 per patient; SD = 37.6 ; n = 15) (Additional File 5). Of these imaging tests, only hip/knee x-rays were performed routinely in all patients (1.0 knee x-ray per TKA patient; 2.1 hip x-rays per THA patient). Other imaging tests were performed selectively, and their use was often associated with complication status (p<0.001) (Figure 3; see Additional File 6-7 for the mean number and cost of these tests by complication status).
The pathology tests contributing most to overall cost burden were: electrolytes/urea/creatinine (mean: AU$27.8 per patient), full blood count (mean AU$27.5), liver function tests (mean AU$15.2), calcium/magnesium/phosphate (mean AU$14.8), coagulation studies (mean AU$6), blood culture (mean AU$4.2), arterial blood gas (mean AU$3.9), urine microscopy (mean AU$3.5), vancomycin-resistant enterococci (VRE) culture (mean AU$3.0) and urine culture (mean AU$3.0) (Additional File 5). Each patient received at least one set of blood tests including electrolytes/urea/creatinine, full blood count and calcium/magnesium/phosphate. The use and cost per patient of all pathology tests increased significantly with the presence and severity of complications (p<0.001; Figure 4).
Figure 3. Largest contributors of imaging cost: cost per patient by complication status.
Figure 4. Largest contributors of pathology cost: cost per patient by complication status
{kind=link}