Patients
[18F]GE180 PET scans of 88 recurrent glioma patients were evaluated. Median age was 49 years (range 23.6–71.9). 56 (63.6%) patients were male, 32 female (36.4%). 42 (47.7%) tumors were diagnosed as IDH-wildtype glioblastoma, 46 (52.3%) as IDH-mutant glioma. Among all 28 IDH-mutant astrocytoma, 10 were classified as WHO grade 4, 17 as WHO grade 3 and one as WHO grade 2, respectively. 18 tumors were classified as oligodendroglioma, IDH-mutant, and 1p/19q-codeleted, 11 WHO grade 3 and 7 WHO grade 2.
Median follow-up time was 15.6 months (95% confidence interval (CI): 13.3–18.0 months). In 59 (67.0%) cases, tumor recurrence was verified histologically, in all other cases, further clinical course confirmed tumor recurrence. All cases of low-grade tumors with new contrast enhancement or new [18F]FET enhancement were histologically verified to prove or rule out malignant transformation. Radiotherapy was performed in 60 cases (68.2%), 26 of them (29.5% of all patients) in combination with chemotherapy. Chemotherapy alone was administered in 22 cases (25.0%), 15 (17.0%) patients received an open tumor resection, 3 (3.4%) received other/experimental treatment and 3 received best supportive care due to clinical deterioration or refusing therapy. Binding affinity status was available for 78 patients; of these, 7 (9.0%) were low-affinity binders, 27 (34.6%) were medium-affinity binders, and 44 (56.4%) were high-affinity binders.
PET Specifications According to Patient Groups
SUVmax values were correlated with CNS WHO grade (Table 1). No significant difference was found between recurrent IDH-mutant and IDH-wildtype tumors.
Table 1
[18F]GE180 uptake characteristics in the examined patient population.
| All recurrent gliomas | SUVmax (median (range)) | P-value |
| Overall (n = 88) | 1.68 (0.59–4.36) | |
| Male (n = 56) Female (n = 32) | 1.73 (0.59–3.83) 1.56 (0.59–4.36) | 0.370 |
| CNS WHO grade 2 (n = 8) CNS WHO grade 3 (n = 28) CNS WHO grade 4 (n = 52) | 0.90 (0.59–3.83) 1.45 (0.59–3.82) 1.91 (0.85–3.83) | 0.031 |
| IDH-mutant (n = 46) IDH-wildtype (n = 42) | 1.60 (0.59–4.36) 1.89 (0.85–3.83) | 0.071 |
| IDH mut. -1p/19 codel (n = 28) IDH mut. +1p/19 codel (n = 18) | 1.72 (.59-3.79) 1.28 (.61-4.36) | 0.714 |
| IDH wt, TERT wildtype (n = 5) IDH wt, TERT mutant (n = 22) | 1.70 (1.29–3.83) 1.89 (1.00-3.12) | 0.909 |
| IDH wt, MGMT methylated (n = 19) IDH wt, MGMT unmethylated (n = 22) | 2.29 (0.85–3.83) 1.81 (1.00-3.03) | 0.114 |
| Low-affinity binding status (n = 7) Medium-affinity binding status (n = 27) High-affinity binding status (n = 44) | 2.32 (0.80–3.79) 1.76 (0.59–3.08) 1.58 (0.61–3.83) | 0.231 |
| SUVmax – maximum standardized uptake value, CNS WHO – World Health Organization Classification of Tumors of the Central Nervous System, IDH – isocitrate dehydrogenase, TERT – telomerase reverse transcriptase |
Post-recurrence treatment
Among all 42 patients with IDH-wildtype tumors, 3 patients with a lower SUVmax and 2 patients with a higher SUVmax received an open tumor resection as part of their recurrence treatment (p = 0.892). Among patients with IDH-mutant tumors, 7 with a lower SUVmax and 3 with a higher SUVmax received an open tumor resection (p = 0.355). Systemic post-recurrence therapies did not differ between patients with a lower or higher SUVmax (p = 0.215 for IDH-wildtype, p = 0.302 for IDH-mutant tumors, Table 2).
Table 2
Treatment regimens in patients with lower or higher than median SUVmax.
| | SUVmax ≤ median (n; %) | SUVmax > median (n; %) | P-value |
| IDH-wildtype (n = 42) Radio-and chemotherapy Radiotherapy only Chemotherapy only Experimental/others No tumor-specific therapy | 21 (100) 7 (33.3) 7 (33.3) 4 (19.0) 0 (0.0) 3 (14.3) | 21 (100) 5 (23.8) 8 (38.1) 6 (28.6) 2 (9.5) 0 (0.0) | 0.215 |
| IDH-mutant (n = 46) Radio-and chemotherapy Radiotherapy only Chemotherapy only Experimental/others | 23 (100) 7 (30.4) 12 (52.2) 4 (17.4) 0 (0.0) | 23 (100) 7 (30.4) 7 (30.4) 8 (34.8) 1 (4.3) | 0.302 |
| SUVmax – maximum standardized uptake value, IDH – isocitrate dehydrogenase |
Post-recurrence survival and time to treatment failure
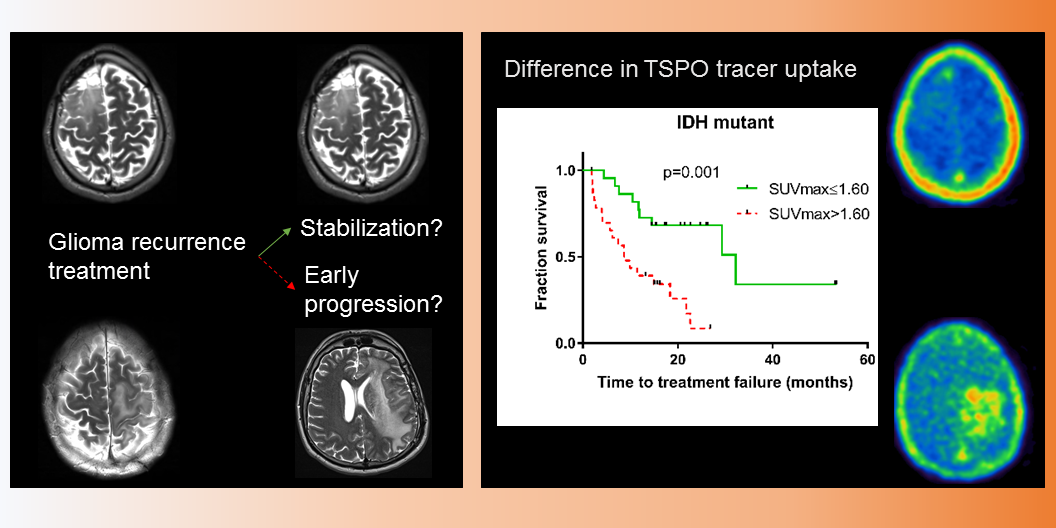
Overall, uptake intensity on TSPO PET at recurrence was highly associated with patients’ outcome: patients with low SUVmax (≤ 1.68; median split) survived more than three times longer than those with high SUVmax (median 41.6 vs. 12.6 months; p < 0.001). Also, the TTF was significantly longer in cases with low SUVmax (14.9 vs. 6.2 months; p < 0.001). Other significant factors in the univariate analysis were IDH and CNS WHO grade for TTF (both p < 0.001) and PRS (p < 0.001 and p = 0.001). In the multivariate analysis, SUVmax remained an independent significant factor for PRS (p = 0.027) and TTF (p = 0.032), whereas CNS WHO grade (p = 0.016) was the only other independent factor for TTF. Accordingly, the association between uptake intensity on TSPO PET and outcome was likewise found in the subgroups of molecularly defined tumors: for patients with recurrent IDH-wildtype tumor, median PRS after recurrence was 8.2 months for patients with an SUVmax higher than the median of 1.89, and not reached for patients with a lower SUVmax (p = 0.002). TTF after recurrence was 6.1 months (6.8 vs. 5.4 months, p = 0.142).
Among patients with IDH-mutant tumors, median PRS was 36.9 months and TTF was 18.4 months. PRS was significantly longer in patients with low SUVmax (≤ 1.60; median split; 41.6 vs. 25.3 months, p = 0.031, see Fig. 1). This difference was also found for TTF (32.2 vs 8.7 months, p = 0.001), also in the subgroups of all astrocytoma, IDH-mutant, and even within the very homogeneous subgroup of CNS WHO grade 3 astrocytoma, IDH-mutant. The small subgroup of oligodendroglioma, IDH-mutant and 1p/19q codeleted, did not have enough events for a separate statistical evaluation (see Table 3).
Table 3
Survival of recurrent glioma patient groups according to tracer uptake.
| All recurrent glioma cases | PRS (median; months) | P-value | TTF (median; months) | P-value |
| All diagnoses (n = 88) SUVmax ≤ 1.68 (n = 44) SUVmax > 1.68 (n = 44) | 27.9 41.6 12.6 | < 0.001 | 8.7 14.9 6.2 | < 0.001 |
| All IDH-wildtype (n = 42) SUVmax ≤ 1.89 (n = 21) SUVmax > 1.89 (n = 21) | 10.6 Not reached 8.2 | 0.002 | 6.1 5.4 6.8 | 0.142 |
| All IDH-mutant (46) SUVmax ≤ 1.60 (n = 23) SUVmax > 1.60 (n = 23) | 36.9 41.6 25.3 | 0.031 | 18.4 32.2 8.7 | 0.001 |
| All astrocytoma, IDH-mutant (28) SUVmax ≤ 1.72 (14) SUVmax > 1.72 (14) | 27.9 36.9 13.5 | 0. 009 | 11.7 22.6 6.2 | 0.007 |
| Astrocytoma WHO grade 3, IDH mutant (17) SUVmax ≤ 1.55 (9) SUVmax > 1.55 (8) | 36.9 36.9 13.1 | 0.015 | 11.7 32.2 2.7 | 0.025 |
| All low-grade (2 or 3) astrocytoma, IDH-mutant (18) SUVmax ≤ 1.33 (9) SUVmax > 1.33 (9) | 36.9 36.9 13.1 | 0.003 | 14.5 32.2 6.2 | 0.063 |
| All oligodendroglioma, IDH-mutant and 1p/19q codeleted (18) SUVmax ≤ 1.28 (9) SUVmax > 1.28 (9) | Not reached Not reached Not reached | 0.464 | Not reached Not reached 18.4 | 0.147 |
| SUVmax – maximum standardized uptake value, IDH – isocitrate dehydrogenase; PRS – post recurrence survival; TTF – time to treatment failure |
Subgroup analyses
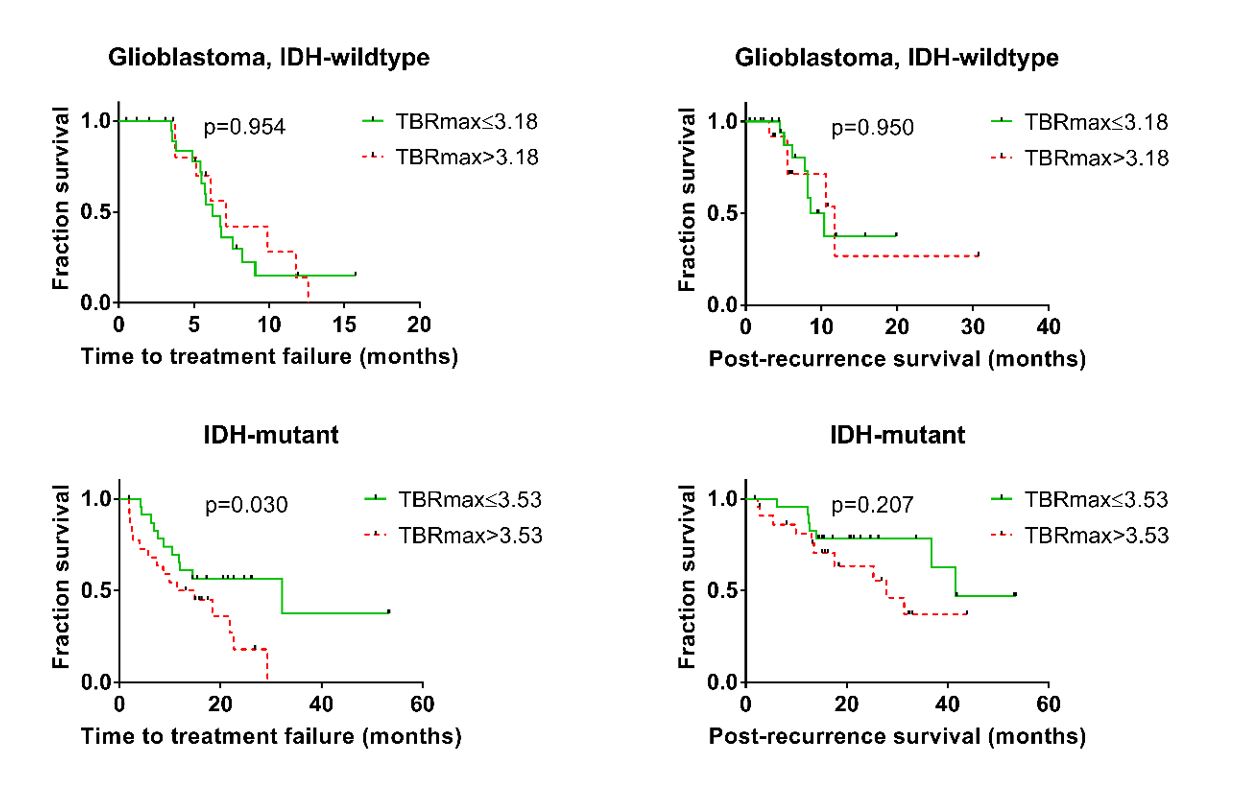
Among patients with IDH-wildtype glioma and a high [18F]GE180 SUVmax, slightly more tumors were MGMT-methylated than in the subgroup of patients with a lower SUVmax (Table 4). MGMT-methylated tumors tended to be treated with chemotherapy, either alone or combined with radiotherapy, more often than unmethylated tumors (63.2% vs 45.5%, p = 0.257). In the 35 IDH-wildtype tumors for whom additional [18F]FET PET was available, [18F]FET TBRmax was higher in the subgroup with high [18F]GE180 uptake, while [18F]FET PET based volume did not differ significantly. Inversely, no significant difference in TTF (p = 0.954) or PRS (p = 0.950) could be seen between patients with a TBRmax higher or lower than the median of 3.18 (Supplementary Fig. 1).
Table 4
Characteristics of high and low [18F]GE180 uptake groups.
| | SUVmax ≤ median (n; % or median; range) | SUVmax > median (n; % or median; range) | P-value |
| IDH-wildtype (n = 42) Male / female sex MGMT methylated / unmeth. (n = 41) TERT wildtype / mutant (n = 27) Age [18F]FET TBRmax (n = 35) [18F]FET tumor volume ( n = 35) T2 volume Contrast volume | 21 (50.0) 14 / 7 (33.3 / 16.7) 8 / 12 (19.5 / 29.3) 4 / 11 (14.8 / 40.7) 55.5 (32.3–70.0) 3.10 (1.55–4.83) 12.60 (0.0-76.66) 50.80 (0.0-198.10) 3.74 (.27-66.2) | 21 (50.0) 15 / 6 (35.7 / 14.3) 11 / 10 (26.8 / 24.4) 1 / 11 (3.7 / 40.7) 55.8 (30.8–70.2) 3.44 (2.47–5.28) 28.71 (4.49-124.75) 80.10 (8.09–337.3) 16.50 (0.0-85.6) | 0.739 0.427 0.223 0.858 0.045 0.109 0.075 0.022 |
| IDH-mutant (n = 46) Male / female sex CNS WHO grade 2 / 3 / 4 MGMT methylated / unmeth. TERT wildtype / mutant (n = 28) Age [18F]FET TBRmax (n = 42) [18F]FET tumor volume (n = 42) T2 volume Contrast volume | 23 (50.0) 12 / 11 (26.1 / 23.9) 7 / 15 / 1 (15.2 / 32.6 / 2.2) 20 / 3 (43.5 / 6.5) 9 / 5 (32.1 / 17.9) 47.5 (23.6–66.2) 2.51 (1.21–5.29) 5.14 (0.0-100.87) 50.7 (13.90-226.50) 0.06 (0.0-12.70) | 23 (50.0) 15 / 8 (32.6 / 17.4) 1 / 13 / 9 (2.2 / 28.3 / 19.6) 18 / 5 (39.1 / 10.9) 10 / 4 (35.7 / 14.3) 39.8 (29.1–71.9) 4.15 (2.88–7.49) 33.08 (1.67-172.04) 59.15 (9.13–253.90) 10.10 (0.0-61.2) | 0.369 0.004 0.437 0.686 0.456 < 0.001 0.002 0.303 0.002 |
| Astro, IDH mut., grade 3 (n = 17) Male / female sex MGMT methylated / unmeth. Age [18F]FET TBRmax [18F]FET tumor volume T2 volume Contrast volume | 9 7 / 2 (41.2 / 11.8) 7 / 2 (41.2 / 11.8) 45.1 (29.9–56.3) 2.01 (1.56–3.82) 3.21 (0.00-71.96) 39.10 (15.70-226.50) 0.00 (0.00-12.20) | 8 6 / 2 (35.3 / 11.8) 5 / 3 (29.4 / 17.6) 37.4 (30.4–57.6) 4.91 (3.08–5.86) 78.87 (11.44-172.04) 63.50 (12.40-110.10) 16.04 (3.84–61.20) | 0.893 0.490 0.198 0.001 0.016 0.842 0.013 |
| SUVmax – maximum standardized uptake value, IDH – isocitrate dehydrogenase, TERT – telomerase reverse transcriptase, [18F]FET – [18F]Fluoroethyltyrosine, TBRmax – maximum tumor-to-brain-ratio, CNS WHO-World Health Organization Classification of Tumors of the Central Nervous System |
In IDH-mutant glioma both [18F]FET volume and TBRmax (n = 42) as well as contrast-enhancing volume on MRI (n = 47) differed between patients with a high or low [18F]GE180-uptake (Table 4). Similar results were found in the subgroup of patients with grade 3 astrocytoma, IDH-mutant. Patients with IDH-mutant glioma and a high [18F]FET TBRmax had a shorter TTF, but no significantly different PRS compared to patients with a low [18F]FET TBRmax (Supplementary Fig. 1).
Among all patients, there was a low to moderate correlation between [18F]GE180 SUVmax and both [18F]FET tumor volume (r = 0.490, p < 0.001), volume in contrast enhanced MRI (r = 0.474, p < 0.001), and T2 MRI volume (r = 0.299, p = 0.006).
{kind=link}
{kind=link}