We performed a prospective study of surgical cases from a single center. The local institutional review board approved this study. Between the years 2014–2015, one fellowship trained foot and ankle surgeon performed all procedures. Inclusion criteria for this study were: (1) patients with mild to moderate hallux valgus as defined by IMA ≥ 9° and < 13°, (2) no previous surgical treatment for hallux valgus, (3) patients 18 years of age or greater, (4) patients indicated for procedures to address alterations in the IMA without simultaneous procedures addressing additional pathology.
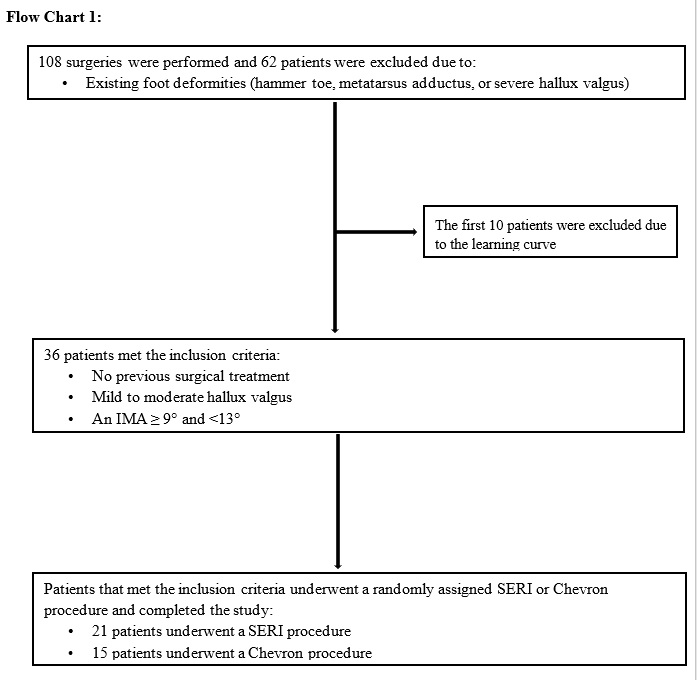
One hundred and eight surgeries were performed for hallux valgus during the study period. Sixty-two patients were not eligible for randomization as they had additional pathology which required surgical intervention at the time of the procedure. Additionally, the first 10 patients who underwent a SERI technique correction of hallux valgus were excluded to account for the surgeon’s learning curve. Ultimately, thirty-six patients who presented during the study period had mild-moderate hallux valgus without additional foot pathology requiring surgical correction and were eligible for inclusion (Flow Chart 1).
Patients indicated for isolated treatment of mild to moderate hallux valgus were randomized using a standard random number generator. The first patient randomized for the surgery day, SERI technique was performed. The surgeon then had time to template the procedure using the PACs system and templating software in the operating room prior to surgery. Twenty-one patients were selected for the SERI minimally invasive procedure and fifteen patients were selected for the standard Chevron osteotomy procedure.
Preoperative Evaluation
The diagnosis of mild to moderate hallux valgus was made via clinical evaluation and standing radiographs. The radiographic measurements and angles recorded included IMA, HVA, and DMMA (Figs. 1–2).
Surgical Procedure
The direction of the osteotomy was determined based on the previously used technique by Kadakia AR at el 4. In order to avoid dorsal head elevation of the metatarsus, the osteotomy was oriented at 10–15° in a plantar direction relative to a plane perpendicular to the metatarsal long axis, from dorsal-distal direction to plantar-proximal direction. And at 10–15° from medial-proximal to lateral-distal direction, in order to prevent shortening of the metatarsal bone length during the recovery period (Fig. 3). Finally, the osteotomy was completed by a manual fracturing of the metatarsals’ lateral cortex in order to preserve the vascular supply, followed by the insertion of a small curved grooved-lever osteotome into the medullary canal of the proximal metatarsal fragment (Fig. 4). Next, the metatarsal head was laterally displaced (Fig. 3) until a percutaneous medial KW could be advanced into the metatarsal medullary canal, adjacent to the grooved-lever osteotome (Fig. 4). The different steps of the procedure were done with the use of fluoroscopy to verify hardware positioning and desired fragments alignment. Finally, the small skin incision was irrigated and closed with a 2/0 absorbable Vicry™ETHICON suture. Wound dressing was done using a gauze pad soaked in an iodine solution, over the metatarsus’s lateral side to overcorrected position of the first toe. Similarly, a semilunar shaped gauze pad was added to the plantar area distally and proximally to the metatarsal cut, in order to decrease the risk of dorsal displacement of the fragment during the recovery period.
The chevron osteotomy was performed using a distal dorsomedial approach to the metatarsal head. When instability of the metatarsal head was observable, a 3.5 cannulated screw was inserted in order to secure the osteotomy.
Post-operative Rehabilitation And Evaluation
Patients in the SERI group and Chevron osteotomy group received a similar postoperative protocol to that described by Giannini et al 1. After the operation, immediate weight bearing was allowed with a DARCO MedSurg™ shoe for 4 to 6 weeks, until signs of bone healing appeared on radiographs. Two weeks after the surgery, the wound was examined and redressed for an additional two weeks. A second postoperative visit at 4–6 weeks included wound examination and oblique and anterior-posterior (AP) standing radiographs of each foot to record the IMA, HVA, and DMMA (Figs. 1–2). Radiographs were additionally used to check for complications, such as osteonecrosis, non-union, or malunion. Three more consecutive postoperative visits were respectively performed at 3, 6, and 12 months, which also included standing radiographs of each foot. The KW was removed 4–5 weeks after surgery depending on the patient’s age, smoking habits and radiographic results. An OrthoWedge™Darco surgical shoe was worn for 6 weeks after the surgery and a regular shoe was permitted to be worn 1–2 weeks after the KW was removed. Patients completed the AOFAS scoring system at the final follow-up appointment.
Statistical Analysis
The statistical analysis was performed using a Fisher exact tests or a Chi-squared test at a significance level of P-value < 0.05. All measured angles (IMA, HVA, and DMMA) were expressed as a mean and standard deviation of the mean. A one-way ANOVA to study the differences between preoperative and postoperative data was performed at follow-up. Statistical analysis was performed using IBM Statistical Package for the Social Sciences (SPSS) Statistics, version 21 for Windows (SPSS, Chicago, IL).
{kind=link}