A total of 19,979 Panoramic radiographs were evaluated from August 2015 till Dec 2021 of which 7,768 were excluded for being duplicate radiographs taken as part of follow-up, further 9,573 radiographs were excluded as lack of CBCT co-relation/maxillary scans. Finally, 2,638 patients having undergone CBCT assessment of the mandibular region for various reasons involving bone evaluation for implant placement and pathologic lesion exclusion were considered. Further 470 scans out of 2,638 (Figure 2) were excluded because of insufficient quality, a low field of view size, normal structural variations like Medial sigmoid depression (MSD), images with artifacts, fracture, or pathologies in the posterior region of the mandible. Each author did the screening independently to reach a final consensus.
All procedures followed were per the protocol of the work centre and ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. This study was approved by the ethical board with vide approval number 20-242E.
Panoramic radiography parameters:
All panoramic radiographs were acquired using Picasso Trio SC 12*7, 3 in 1 system with integrated EzDent software having technical parameters: Image volume size 12 x 7 cm, D-051 stationary anode type tube, tube current 2-10 mA, tube voltage 40 - 90 kV, focal spot 0.5 mm, total filtration 2.8 mm Aluminum, exposure time 11.3 s / 13.2 s.
Cone beam computed tomography parameters:
The basic mandible reconstruction was performed based on volumetric methods of scanning using 3D CBCT by Orthopantomograph OP300 scanner with technical parameters: image volume size 80 × 150 mm, tube current 15 mA, tube voltage 80 kV, scan time 16 s, exposure time 12 s pulsed X-ray was used for all images.
The software used was DICOM OnDemand3D from Cybermed, USA, for the reconstruction of sagittal, axial, coronal, and three-dimensional images. Image acquisition and scans were reported and consulted by three specialists with at least two-decade experience in their respective fields of Maxillofacial radio diagnosis, medical imaging, and Head & Neck imaging to rule out the MSD, other possible pathologies and to rule out the occurrence of pseudo foramina or a pseudocyst as a post-acquisition or manipulation error in doubtful cases. All evaluations were performed on a 15.6-inch monitor with a resolution of 1366 x 768.
Statistical analysis:
The data obtained were analyzed using Statistical software SPSS 2.2.0 and R environment 3.2.2. Descriptive and inferential analysis was done. Based on the available data the following assumptions were considered: Dependent variables should be normally distributed, Scans drawn from the patients were random and cases of the scans being independent. The recorded variables were the patient's gender, age, distribution pattern, and surface localization of the foramina. The dependent variables were assessed to see if they were normally distributed using a Shapiro-Wilk test.
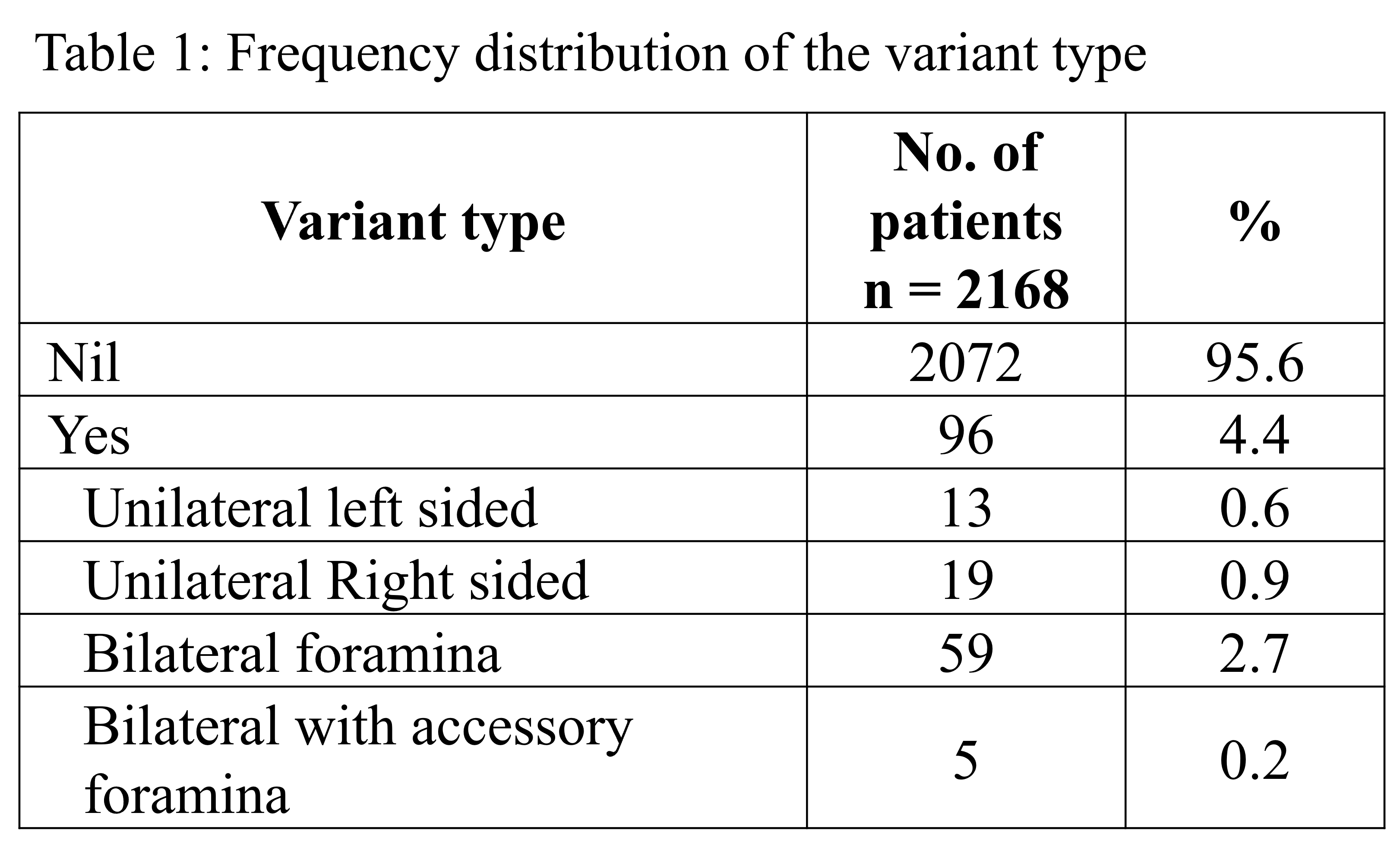
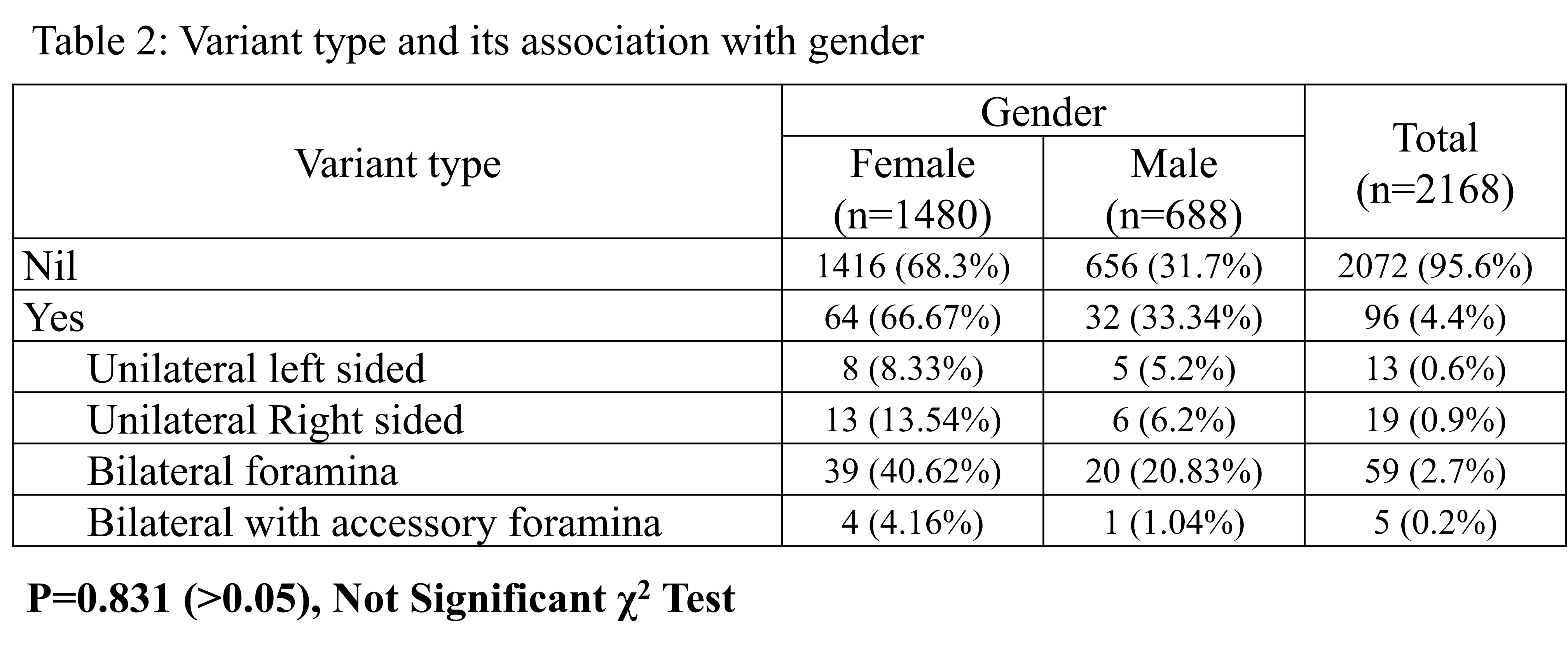
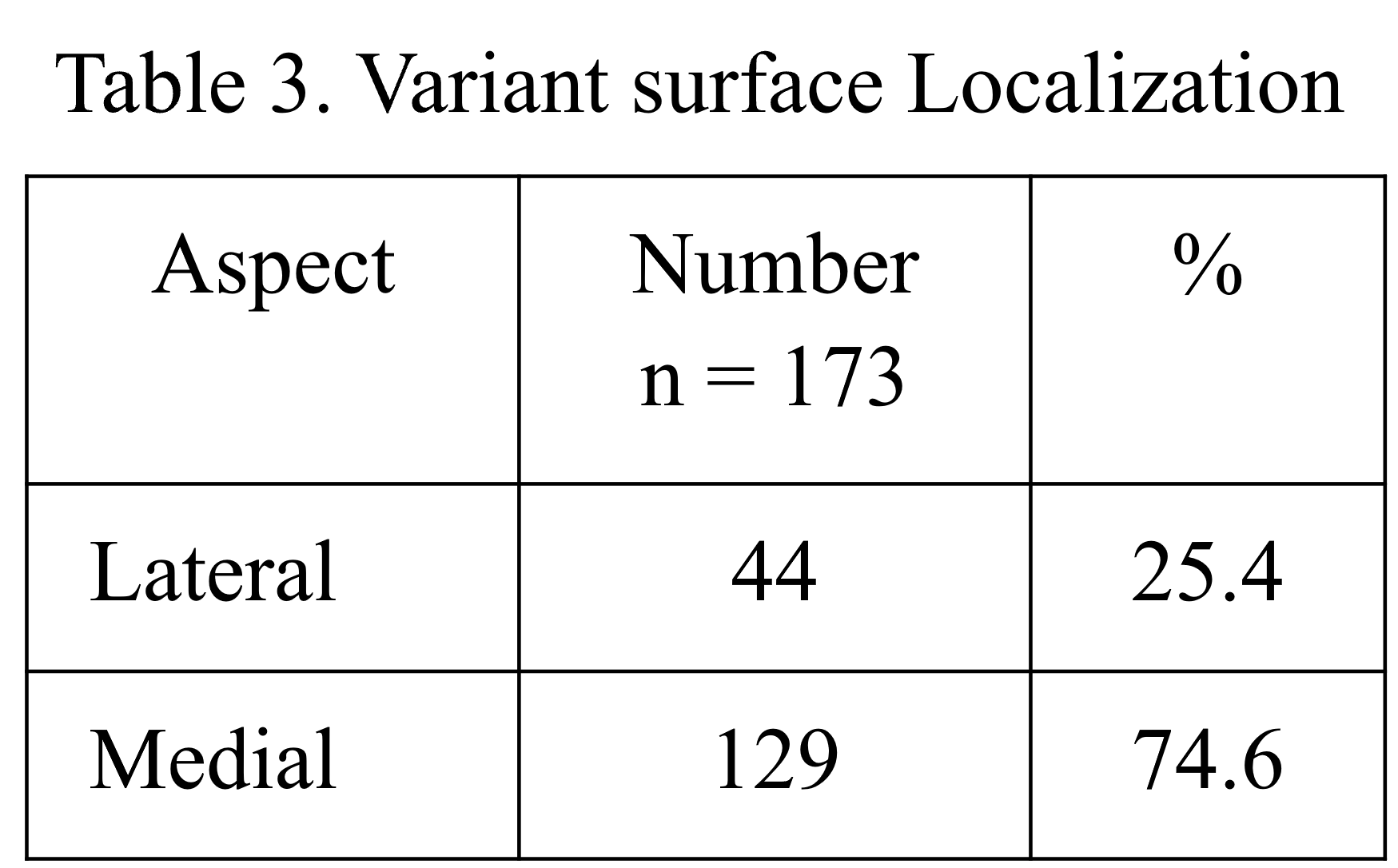
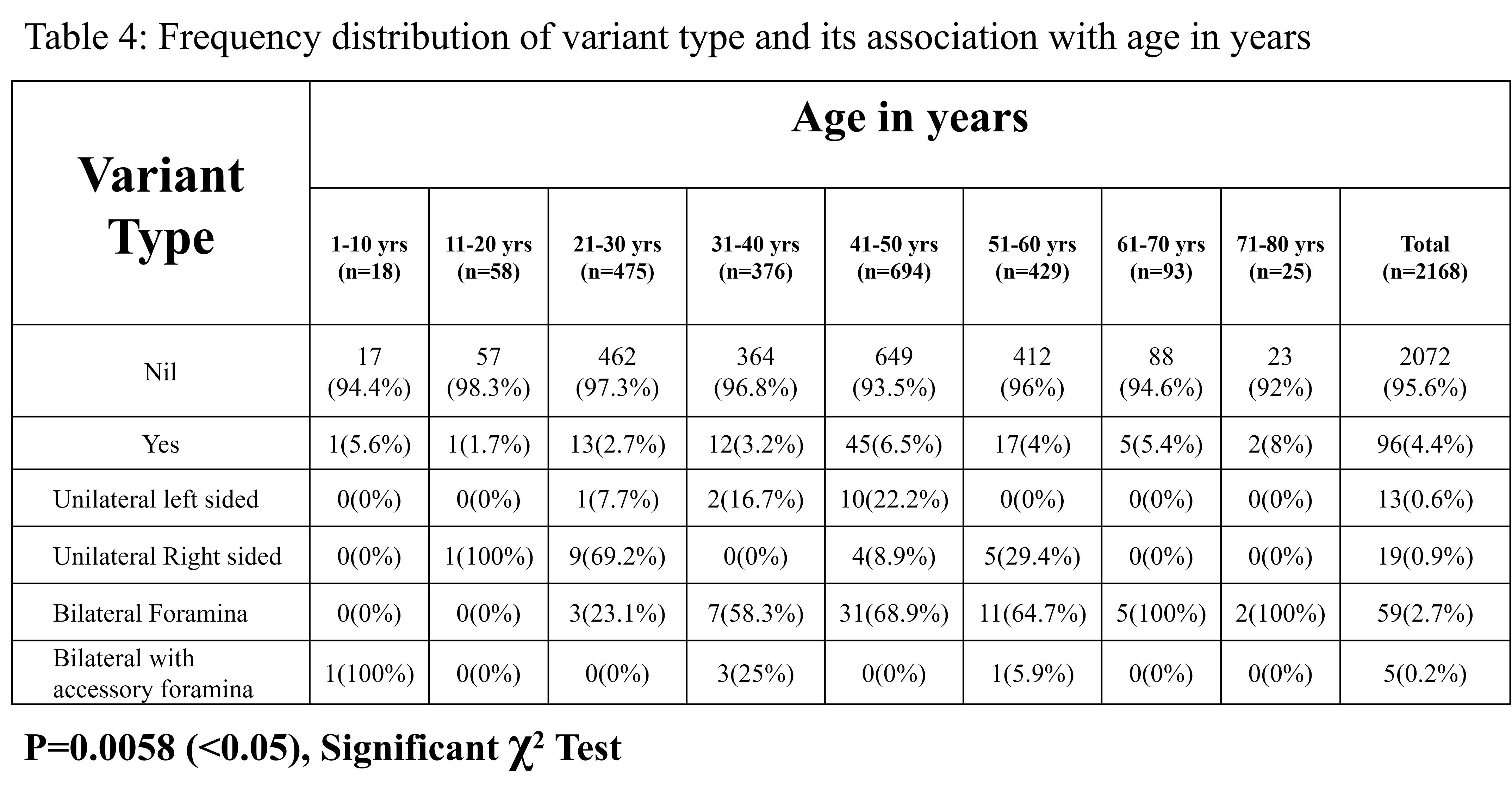
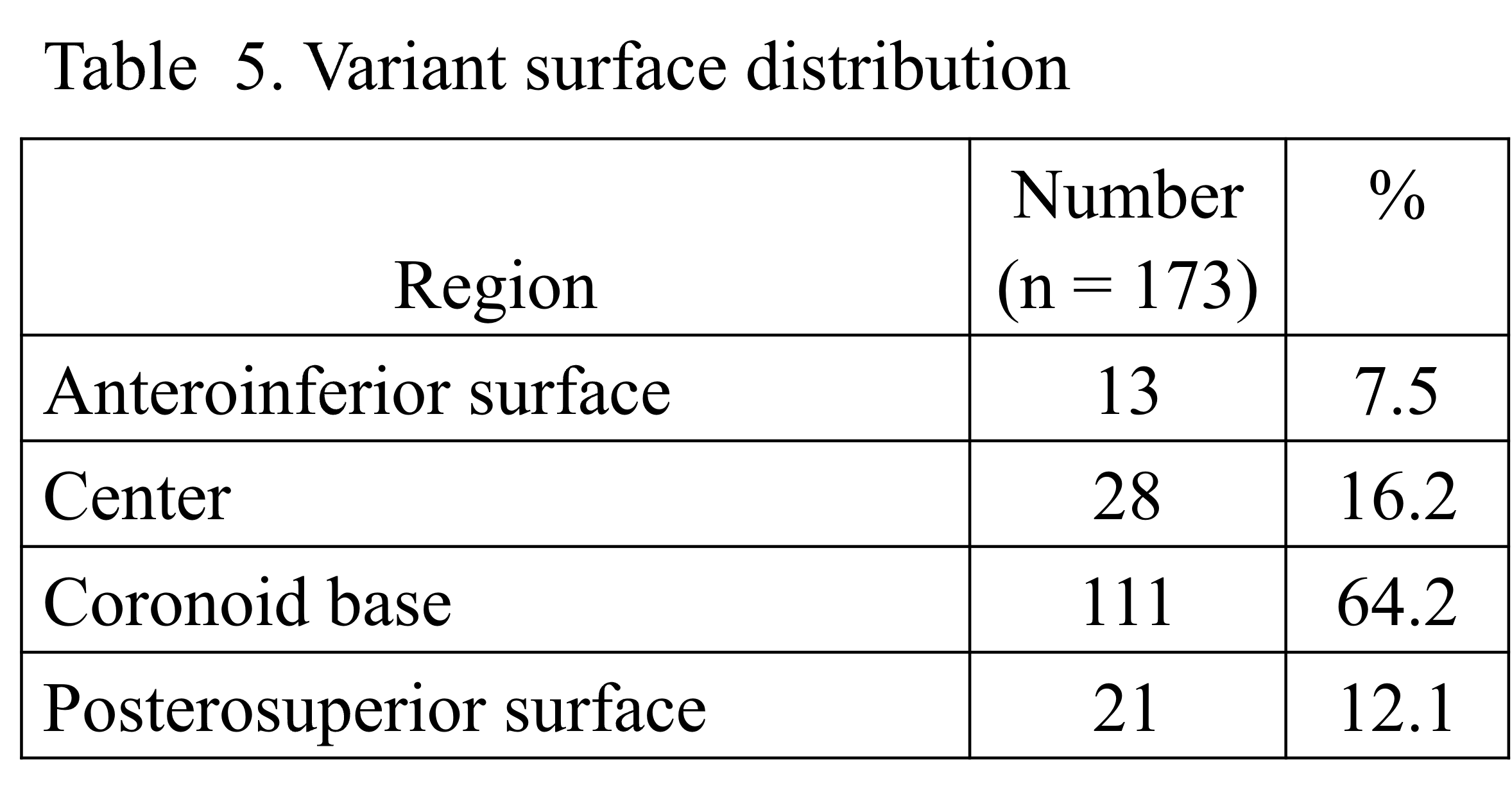
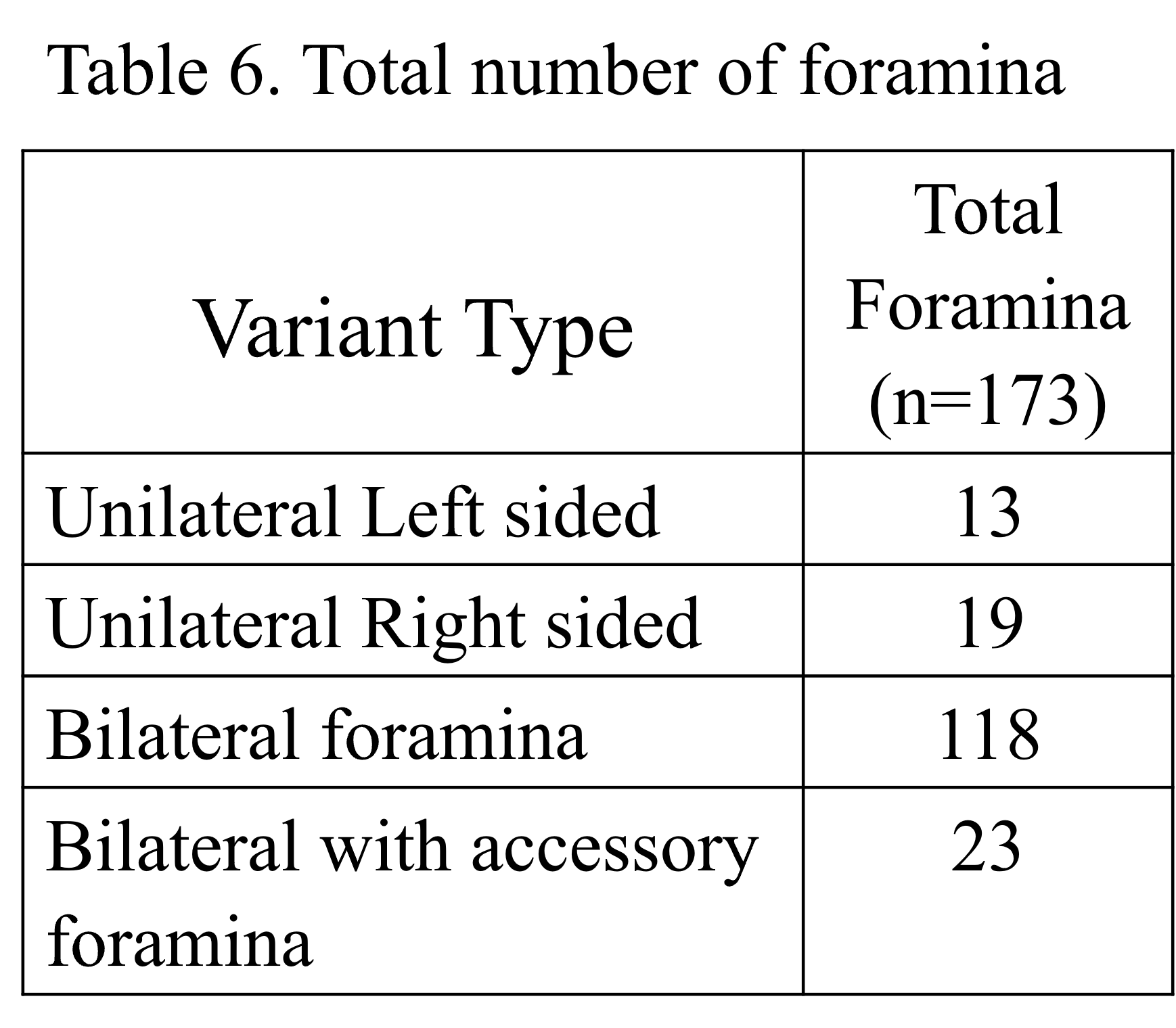
Descriptive statistics such as number, gender, age, and surface localization for the variables are represented in tables (Table 1 - 4). Chi-Square / Fisher Exact test was used to find the significance of study parameters on a categorical scale between two or more groups & a non-parametric setting for qualitative data analysis was done. The Fisher Exact test was used when cell samples were small while investigating the normal distribution of the variables. On the interpretation of the results, the level of significance was set at 0.05; in the case of p<0.05, there was a significant association between variables, whereas in the case of p>0.05 there was no significant association with the variables on a categorical scale.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}