Study setting and population
A retrospective study was carried out in emergency intensive care unit (EICU) of Zhongshan Hospital, Fudan University, Shanghai, China. Patients diagnosed with sepsis on admission between January, 2014 and January, 2018 were enrolled in this study. The diagnosis of sepsis referred to The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) , namely suspected infection with Sequential Organ Failure Assessment (SOFA) score ≥ 2 [2]. Information of infection and SOFA score were acquired from Electronic Medical Record System (EMRS). Patients were excluded if they had one of the following conditions: ① under the age of 18; ② suffering chronic heart failure (New York Heart Function Assessment - IV), advanced malignancy, end-stage liver (Child-Pugh C) or kidney diseases (CKD-5); ③ having received in-hospital treatment in other hospitals prior to admission; ④ in-hospital LOS less than 48 hours. Anti-infection treatments of included patients were applied by experienced physicians based on either etiological evidence or empirical therapy plan. The study was approved by the Ethics Committee Study Board of Zhongshan Hospital, Fudan University (record number: 2006-23).
Diagnosis of secondary infection
Secondary infection was diagnosed according to CDC/NHSN Surveillance Definition Of Health Care-Associated Infection And Criteria For Specific Types Of Infections In The Acute Care Setting [25]. Clinical information used to identify secondary infection such as signs/symptoms and results of laboratory tests such as pathogen cultures were acquired from EMRS. Only the newly-onset nosocomial infections identified later than 48 hours after admission were classified as secondary infections. The time of the onset of secondary infection was the day when positive cultures were collected, or when signs/symptoms emerged if no positive cultures were gained. Infections identified after leaving hospital were not documented. An infection caused by multiple pathogens but identified at the same time and same site was considered as one infection. Three experienced researchers were responsible for the diagnosis of secondary infection.
Data collection
EMRS and Computerized Physician Order Entry (CPOE) were screened for available data. The following data of each patient were collected: ① baseline characteristics: age, gender, comorbidity and smoking history; ② site of primary infection; ③ index of severity of the disease on admission: Acute Physiology and Chronic Health Evaluation II (APACHE II) score, SOFA score and hemodynamic status; ④ interventions such as the use of glucocorticoids, anticoagulation therapy, mechanical ventilation, urinary catheterization, deep venous catheterization, continuous renal replacement therapy and blood transfusion (whether those interventions were applied before or after the onset of secondary infection was noticed); ⑤ occurrence time, site and pathogen of secondary infection; ⑥ LOS in hospital and ICU, the outcome of hospital stay.
Measurement of monocyte HLA-DR expression and serum levels of cytokines
In order to explore the underlying immune mechanism of secondary infection, we acquired the data from Database of Clinical Sample and Information for Sepsis of Zhongshan Hospital, an database founded in 2008 and intended for the collection and perseveration of clinical samples of septic patients. According to the guideline of database, the peripheral blood samples were collected in the BD Vacutainer® tubes (BD Biosciences, CA, USA) at day 1, 3 and 7 after admission. In some patients, sample at day 3 and 7 were not collected due to specific clinical conditions. Thus, data of only a part of the included patients were available as the limitation of a retrospective study. To explore CD14+ HLA-DR+ monocytes expression, a following double color staining was utilized: a fluorescein conjugated (FITC)-CD14, allophycocyanin conjugated (APC)-HLA-DR (BD Biosciences, CA, USA), according to manufacturer’s instructions. Appropriate isotype controls were run with healthy controls and used for compensation and gating blood samples. Subsequently, samples were analyzed on a 18-parameter BD LSR Fortessa analyzer (BD Biosciences, CA, USA) with FlowJo software (Tree Star Inc, OR, USA). HLA-DR expression was shown as the percentage of CD14+ HLA-DR+ monocytes among all CD14+ monocytes. The levels of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), IL-8 and IL-10 were measured by ELISA method (R&D System, MN, USA) according to manufacturer’s instructions. The experiments of flow cytometry and ELISA were conducted right after the samples were collected and the results were recorded in the database. In this retrospective study, the results were directly acquired from the database.
Statistical analysis
The Kolmogorov-Smirnov test was used to verify the normality of all data. Normally distributed data were expressed as means and standard deviations (SD). Abnormally distributed continuous data were expressed as medians with the 25th and 75th quartiles. Categorical data were expressed as frequency and percentage.
The risk factors of secondary infection of septic patients were explored by a two-step method. Firstly, univariate analysis was conducted. Covariates included age, gender, comorbidities, smoking history, site of primary infection, hemodynamic status and severity of disease on admission, HLA-DR expression, serum cytokines levels and clinical interventions before onset of secondary infection. Student’s t test was used to compare normally distributed data and Mann-Whitney U test was utilized to compare abnormally distributed data. Categorical data were compared by Pearson’s chi-square test or Fisher’s exact test when appropriate. Secondly, covariates with statistical significance in univariate analysis were tested in multivariate binary logistic regression analysis to identify the independent risk factors by means of Backward: Conditional method. Because of the data missing of HLA-DR expression and serum cytokines levels, they were not brought into multivariate analysis. Dynamic changes of HLA-DR expression and serum cytokines levels were also statistically evaluated by comparing the levels of biomarkers between different points in time using Mann-Whitney U test.
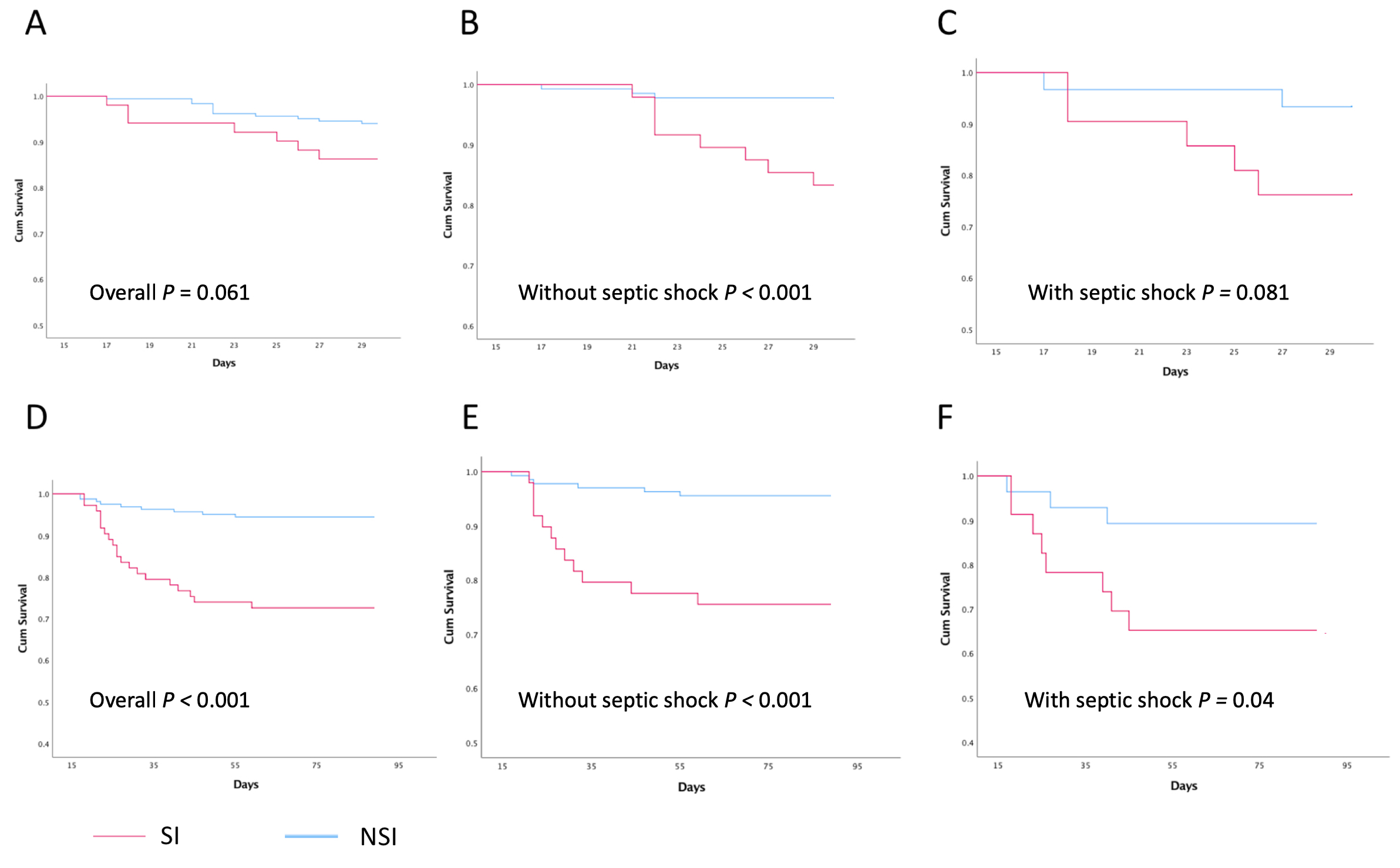
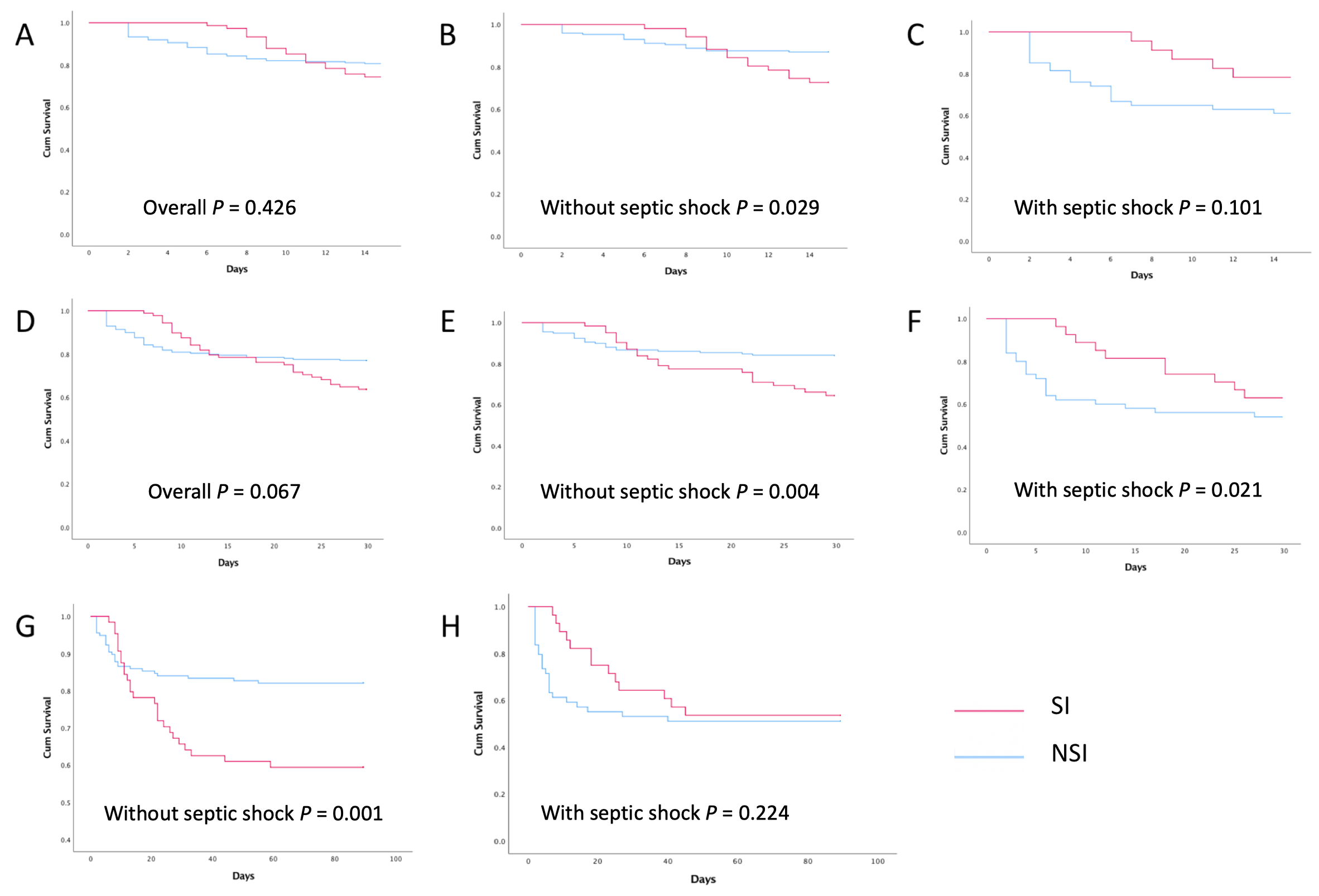
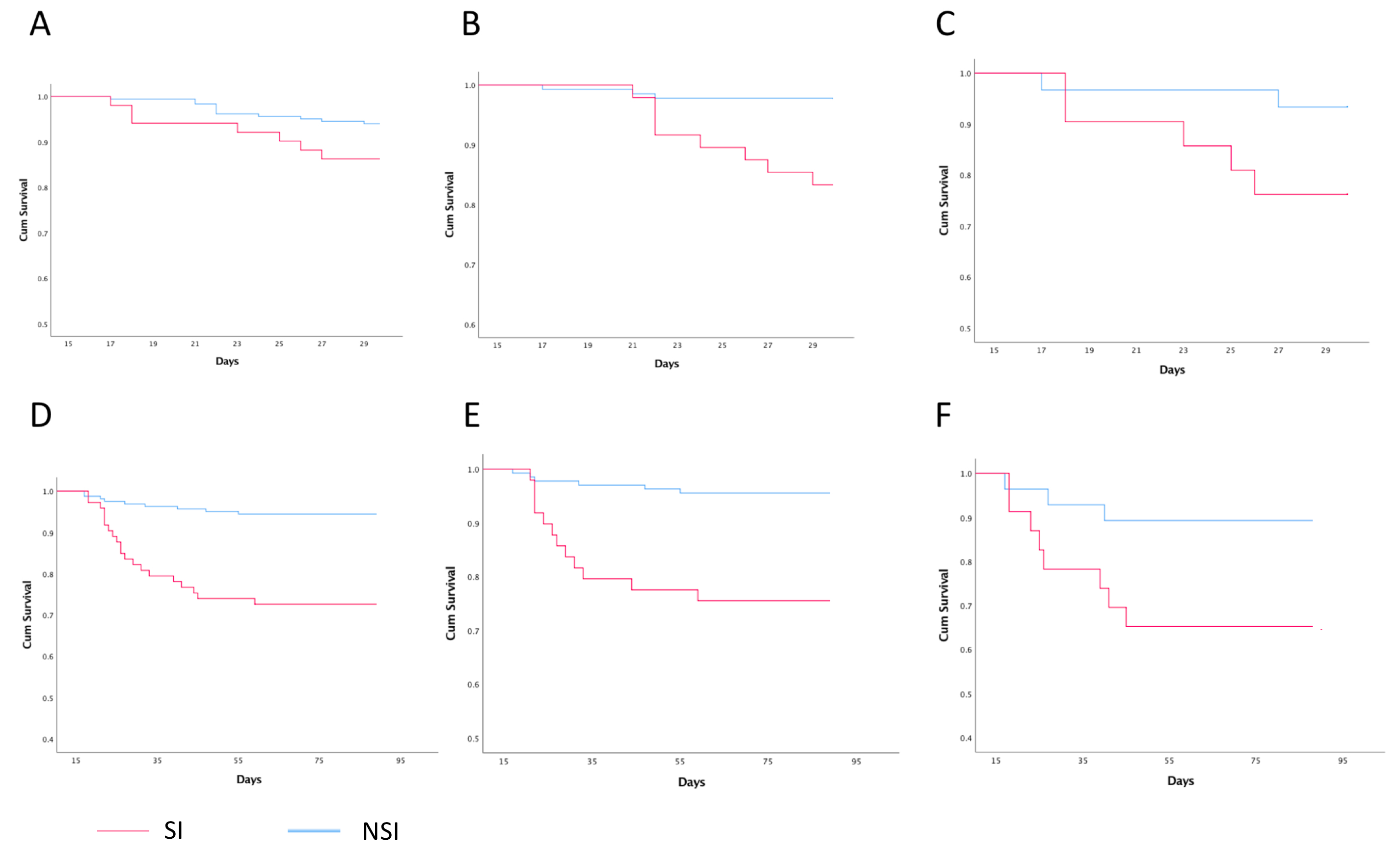
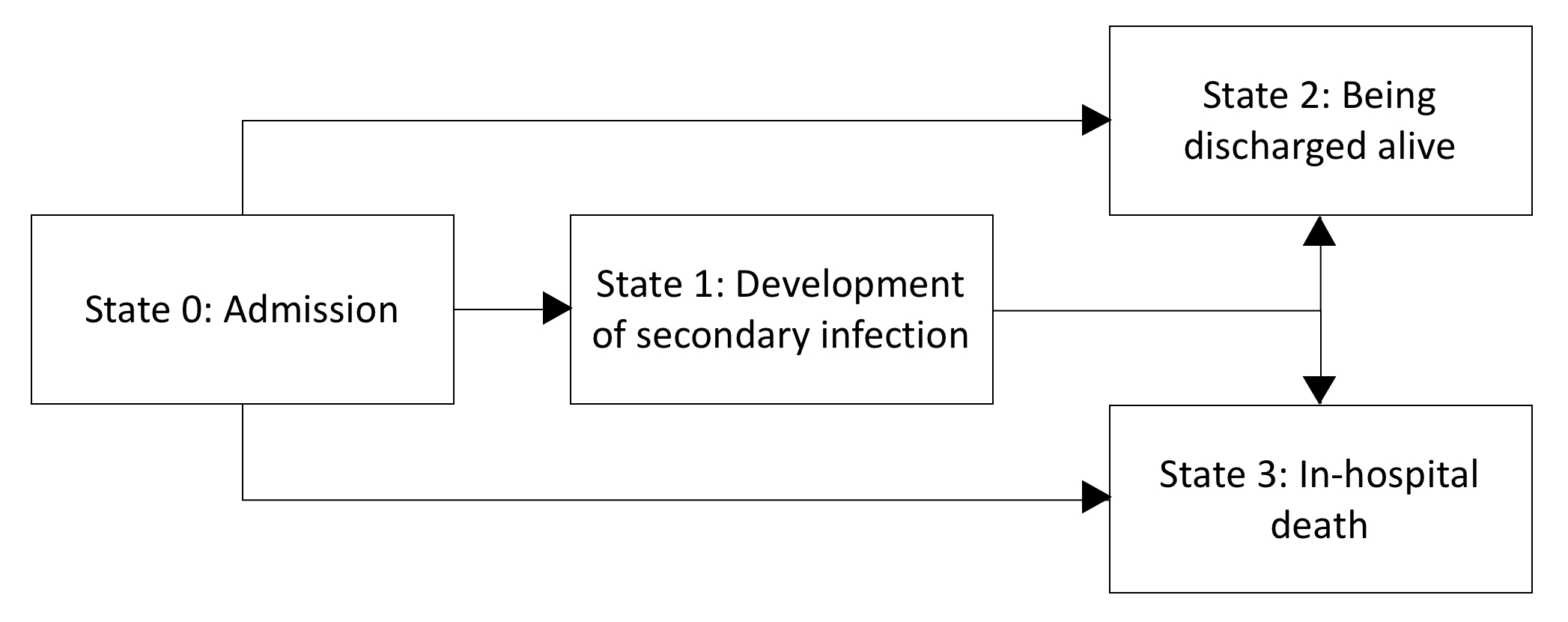
In our study, we treated in-hospital LOS as an outcome of secondary infection, rather than a potential risk factor. A multistate model with 4 states (state 0: admission, state 1: development of secondary infection, state 2: being discharged alive, state 3: in-hospital death) was performed using “etm” package in R in order to explore the influence of secondary infection on in-hospital LOS [3,26], where the data of patients with an in-hospital LOS longer than 100 days were omitted to eliminate the impact of extreme cases (see Additional file 1: Fig. S1). Survival analysis was conducted using Kaplan-Meier method. Log-rank test was used to compare survival curves and it was conducted in every division once two curves had intersections. The two-step method was also used to explore the risk factors of mortality. Univariate analysis was conducted first and followed by multivariate binary logistic regression analysis. Secondary infection was among covariates, together with age, gender, comorbidities, smoking history, site of primary infection, hemodynamic status and severity of disease on admission, clinical interventions and in-hospital and ICU LOS.
All statistical analyses were two-sided, and the significance level was set to P < 0.05. We checked the model assumptions before using each statistical method. Statistical analysis was conducted on SPSS 25.0 (SPSS Inc., IL, USA) and R 3.5.1 (R Development Core Team).
{kind=link}
{kind=link}
{kind=link}
{kind=link}