The widespread use of NOACs has resulted in a significantly lower risk of stroke, systemic embolism, death and intracranial haemorrhage in patients with atrial fibrillation compared to VKAs[28], while the use of NOACs in patients with valvular heart disease remains somewhat disputed. Nevertheless, the evidence which supports the clinical benefit of NOACs in atrial fibrillation combined with left-sided BHV is rapidly growing in recent years. The findings pooled from this study have important implications for the selection of anticoagulants for patients with aortic or mitral BHV and AF who require long-term anticoagulation.
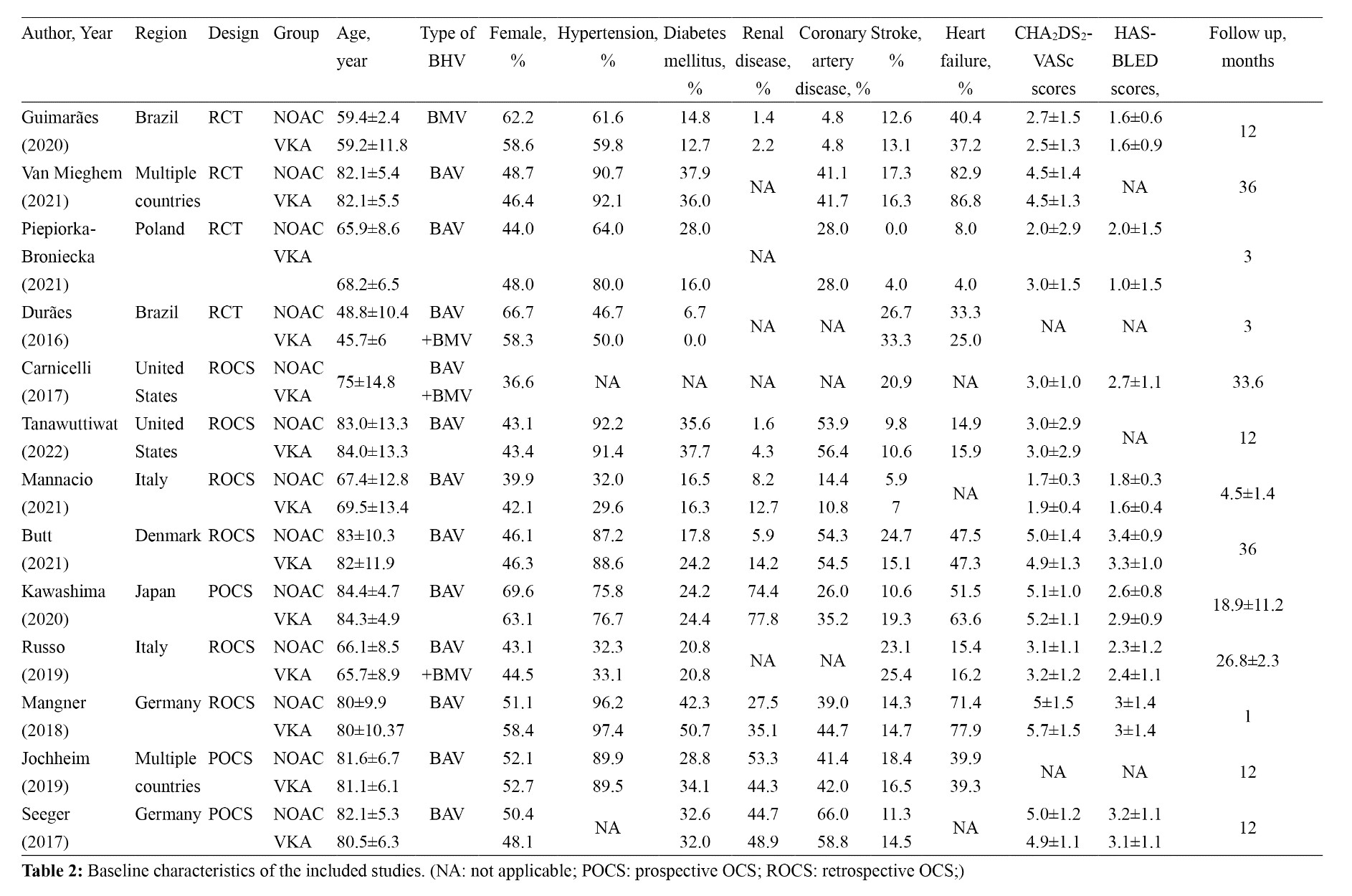
A total of 28,092 patients with previous left-sided BHV replacement and AF are included in our meta-analysis while all of them received either NOACs or VKAs to prevent thrombosis events. The results find that NOACs are not inferior to VKAs in reducing the incidence of stroke, all-cause mortality and any bleeding. Among patients aged less than 80 years, we find that NOACs have a better value for stroke prevention than VKAs, while NOACs might have a better role in reducing the episodes of major bleeding episodes. And NOACs may have even better application in reducing any bleeding in patients without heart failure.
Due to the inherent limitations of OCSs, selection bias in the inclusion of patients with AF and BHV compromises the generalizability and applicability of their conclusions. Limited evidence from large double-blind RCTs researching NOACs versus VKAs in AF and BHV, has led to uncertainty in choosing the appropriate antithrombotic regimen in this group with high risk of stroke. Since older people account for a greater proportion in the population of VHD and AF, patients with AF and BHV recruited in RCTs tend to be healthier, have a higher quality of life, and have fewer comorbidities. In this context, our meta-analysis included both RCTs and observational cohort studies to provide evidence for the anticoagulant effect of NOAC in the real world. And the generation of evidence with large sample sizes will further facilitate the conducting of RCTs.
Stroke prevention is the main reason for the use of anticoagulants in patients with AF, especially in patients with co-existing BMV or BAV[29, 30]. Although our study find that the pooled rate of stroke was similar in NOAC-treated patients compared with those on VKAs in both RCTs and OCSs, the increasing heterogeneity between studies makes its authenticity arguable. To explore the sources of heterogeneity, we analysis the difference between NAOC and VKA in stroke prevention using a cut-off age of 80 years. In the analysis of subgroups less than 80 years, NOACs demonstrate good value in the prevention of cerebral thrombotic events, while the heterogeneity between studies is significantly lower. However, in people older than 80 years, the difference between the two classes of anticoagulants is not significant. The scores of CHA2DS2-VASc are used to determine thresholds for initiating anticoagulation in patients with AF, while age is an important component of it. However, the cut-off scores for starting anticoagulation varies between guidelines, leading to conflicts over the choice of starting anticoagulation in elder patients[6,31−33]. A recent population-based cohort study of 16 351 individuals found a 2.4-fold increased risk of stroke in patients aged 66 to 74 years with AF but no other CHA2DS2-VASc risk factors[34]. This finding also provides support for the need of subgroup analysis according to age and incorporating age into the selection of anticoagulants for AF combined with BHV. Divergence effects across age groups, rather than differences between designs of study and inclusion other population characteristics, explains the statistical heterogeneity observed in the pooled analysis of stroke and suggests that younger patients may benefit more from choosing NOACs over VKAs.
With regard to the efficiency outcomes of all-cause mortality, the RCTs are consistent with the conclusion from the OCSs that there is no significant difference of adverse event rate between patients treated with NOACs and VKAs. Sensitivity analyses in both RCTs and observational cohort studies do not reveal fluctuations towards the results. The large number of patients included in the RCTs lead to a higher level of evidence to support this conclusion[35]. Heterogeneity in OCSs may stem from studies’ inherent differences in comorbidities.
As a significant complication, major bleeding is an important reason why patients with AF combined with BHV are unable to use anticoagulants or have poor compliance with them[36]. Our meta-analysis analyses the effect of NOACs and VKAs on major bleeding events in RCTs and OCSs respectively. The conclusions drawn from these two subgroup analyses are inconsistent. Data from OCSs suggest NOACs reduce major bleeding events compared to VKAs. In contrast, the incidence of major bleeding is not having distinctions in the subgroup of RCTs. The heterogeneity in the subgroup analysis of the RCTs is mainly derived from one single study by Van Mieghem et al[15]. In the sensitivity analysis, we observe a numeric lower incidence of hemorrhage, though not statistically significant (RR 0.48; 95% CI 0.20–1.15; I2 = 0%), and no heterogeneity among studies when omitting this report. This may be explained by the fact that more than 40% of patients in the VKAs group from this study were not adherent to trial drugs during the follow-up period. Given that not all OCSs are designed by propensity matched, the ability of NOACs to reduce the rate of major bleeding, compared to VKAs, remains to be confirmed by future larger RCTs.
In the subgroup analysis of RCTs for any bleeding, we find no meaningful differences between NOACs and VKAs. Differences in the criteria for determining any bleeding may account for part of heterogeneity in OCSs. We also find that any bleeding events due to NOACs appear to be reduced than VKAs in studies with a smaller proportion of patients with heart failure. A randomised controlled study indicates that a higher proportion of liver and kidney disease are found in the patients with heart failure[37]. As important components of the HAS-BLED score, abnormal liver and kidney function also lead to a further increased risk of bleeding after the use of anticoagulants which is in line with our conclusions[38].
There are still some aspects in our meta-analysis which are novel and have potential clinical interest with respect to the existing published reports. First of all, the body of subjects included in our meta-analysis is the largest than others. Due to the low incidence of stroke and major bleeding events, a large sample size provides more robust evidence for physicians. Secondly, patients with both BMV and BAV are included in our study. There is no significant difference in the choice of anticoagulants between the two type of BHV for patients with AF in the current guidelines, despite the differences in the haemodynamic environment in which they are operated[7, 39]. The use of NOACs in BMVs also holds good promising qualities than VKAs. Moreover, our meta-analysis provides a meaningful insight in selecting anticoagulants to prevent stroke for patients who are younger than 80 years and not suffering from heart failure.
{kind=link}