In this study, a specific nomogram was constructed and validated to predict 1-, 2-, and 3-year OS of postoperative patients with LSCC. We performed nomogram variables screening and found seven clinical factors to establish a predictive nomogram for the prognosis of LSCC patients receiving a surgical procedure, as well as risk stratifications. Seven clinical risk factors were age, gender, marital status, T stage, N stage, surgical type, and radiotherapy. In terms of the predictive performance, we conducted ROC curve analysis, calibration curves, and DCA curve, which indicated clinical application value in guiding individualized treatment of patients.
Survival prediction tools, such as the medical nomogram, for postoperative patients with LSCC can play an important role in generating a probability of a clinical event, such as cancer recurrence or death, for a given individual[16]. Recently, a growing number of studies have focused on survival for patients with NSCLC including LSCC and LUAD[17–19]. However, much of the current effort in lung cancer nomogram studies is focused on NSCLC and LUAD[20, 21] because NSCLC accounts for about 85% of lung cancers, with LUAD being the most abundant among the NSCLC subtypes[22]. By contrast, fewer studies have examined the prognosis of LSCC patients. Zhang [23] constructed a nomogram to accurately predict the incidence of brain metastasis in patients with LSCC, which may contribute to the early identification of high-risk LSSC patients and the establishment of individualized treatment. This study focused on the brain metastasis while our study excluded M1, N2, and N3 stage LSCC patients who were not suitable for surgical treatment and focused on the patients’ survival. Zheng [24] performed a nomogram study that had several similarities to ours, which satisfactorily predicted 3-, 5-, and 7-year cancer-specific survival and OS rates for patients with LSCC. This study applied limited methods to evaluate the quality of predicted models and paid attention to all-stage lung cancer patients regardless of whether there were any indications for surgery or not. But it is noteworthy that LSCC and LUAD differ in the composition of genes, molecular characteristics, such as epidermal growth factor receptor gene mutations, and prognosis[25]. Meanwhile, as the low-dose computed tomography screening in lung cancer diagnosis extensively applied, the identification of early-stage lung cancer has increased remarkably, making it possible for lung cancer patients to share more opportunities of a more conservative surgery and a better long-term survival[26, 27]. It may be more reasonable to separately discussed the operable and inoperable LSCC patients as the prognosis of lung cancer patients with different stage varies greatly[28]. Thus, we carried out the first study to predict 1-, 2-, and 3-, OS of postoperative LSCC patients selected from SEER database, which tends to stay close to the clinical problem.
In addition, Li [17] identified eight RNA binding proteins as prognosis-related hub genes, which were used to construct a prognostic nomogram model for overall survival of LUAD patients. Liu [18] found that thirty-three autophagy-associated genes could dichotomize patients with significantly different OS and independently predict the OS in LUAD and LSCC patients, respectively. Most of those nomogram-related prognosis studies applied ROC curve analysis, calibration curves, and DCA curve to assess the predictive performance. Those survival-related nomograms were all based on the information at the transcriptional or translational level. However, sequencing data is relatively difficult to achieve due to the fact that sequencing platforms may be not accessible or economical to all medical institutions and patients. Our predictive nomogram was based on patients’ clinicopathological and demographic characteristics which are more readily accessible to individual health professionals with the wide application of electronic medical record systems.
Multivariable Cox regression analysis showed that seven clinical factors including age, gender, marital status, T stage, N stage, surgical type, and radiation were significantly associated with OS. Among them, patients aged > 77 years presented a significantly higher risk of death than those aged < 67, implying that ageing is a poor prognostic factor for lung squamous cell carcinoma, which is consistent with previous studies[29, 30]. Many studies revealed sex differences existing in survival and female lung cancer patients have higher survival[31, 32]. Our nomogram showed the same result that male was a parameter with a higher score in the nomogram, which was negatively correlated with survival probability. As for marital status, several reports suggested it was significantly associated with survival in patients with lung cancer[33, 34]. TNM stage, well-known prognostic factors, had significant contribution to prognosis for NSCLC patients[35]. The mainstay of treatment of potentially resectable stage I, II, and part III lung cancer patients is surgical removal of the tumor, which includes pneumonectomy, lobectomy, sublobectomy, and so on[36]. Our findings indicated that the nomogram variable lobectomy scored highest of the surgical types, as followed by pneumonectomy and sublobectomy and the nomogram scores was negatively correlated with the prognosis. Lung resection had a significant impact on pulmonary circulation and ventilation, as well as posing a hurdle in terms of elevating survival and different surgical types had differences in long-term survival[37]. For instance, lobectomy has been associated with lower surgical complications and operative mortality rates than pneumonectomy, which may be associated with smaller surgical resection and more normal lung tissue preserved[37]. Some researchers also compared the effect of surgical types on long-term survival of LSCC patients. Gezer [38] performed a retrospective study which indicated that LSCC patients receiving sleeve lobectomy proved to a lower mortality than standard pneumonectomy and resulted in better lung function and quality of life.
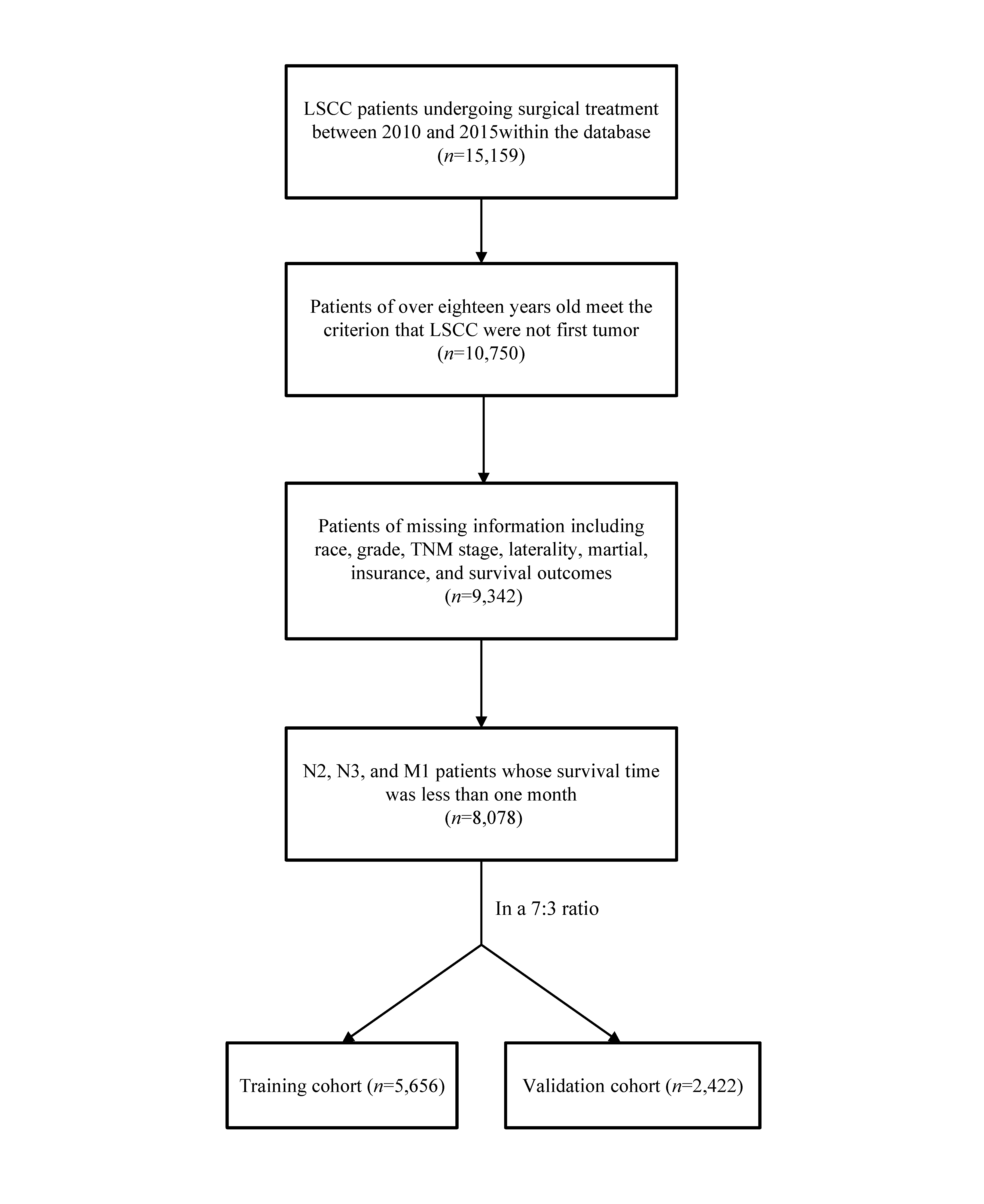
Our study has several strengths. Firstly, this study was the first to establish a long-term predictive nomogram for postoperative LSCC patients based on SEER database. It is worth noting that earlier and more accurate prediction of long-term survival in LSCC patients undergoing lung surgery could provide more time for physicians to offer customized treatment strategies. Secondly, our study had a large sample size including 8,078 LSCC patients, allowing us to clarify an available prognostic model. Thirdly, because our study was a population-based study, our results are representative of real-world clinical practice. Fourthly, compared to nomograms based on genomic data, our nomogram can be more readily adapted to different application scenarios varying from hospitals in smaller and rural communities to high-volume hospitals as a result of more accessible clinical characteristics.
There are several limitations of our study. Firstly, even though the SEER registries include patients from eighteen population-based regions, the data may not be generalizable to other regions not covered by SEER. Therefore, future multicenter and prospective studies are required to prove or disprove these findings. Secondly, nomogram variables derived from SEER database doesn’t cover clinical data such as symptoms and signs, co-morbidities, past cigarette use, recent weight loss, family history of cancer, type of radiotherapy, and occupational exposures, which could bias study findings. In addition, clinical data was not universally reasonable in SEER database. For example, tumor staging in SEER database was based on AJCC 6th and 7th edition TNM classifications which are not in accordance with the 8th edition. Although we updated the T, N, and M stages according to the 8th criteria, it still couldn’t reflect the real clinical situation. It could also lead to selection bias that patients who received and were lack of chemotherapy were classified into the same category. Thirdly, with the assumption that the predictors interact in an additive and linear way, our predictive model was developed using the traditional Cox regression analysis. The predictive power of the nomogram could be limited as a result of ignoring the fact that the interactions between predictors are inherently non-linear and multifactorial[39].
{kind=link}