As with most viral infections, oral symptoms may be observed during COVID-19, although the correlation between these symptoms and the disease has not been conclusively proven. It’s been reported in the literature that oral symptoms have been observed in 68% of the COVID-19 cases(9). It's also been reported that oral symptoms develop at about the same time as respiratory symptoms in mild cases; whereas in severe cases, they occur 1-4 weeks after(4).
A myriad of studies have been published about the significance of ACE2 membrane receptors in the SARS-CoV-2 virus's invasion of a host cell, identifying the tissues that have a higher level of ACE2 expression (lungs, keratinized areas of the oral mucosa) as „target sites“, and emphasizing the potential role of saliva in diagnosis (7, 10, 11). It’s been stated that elevated ACE2 expression in alveolar tissues, oral and oropharyngeal mucosal cells, the gastrointestinal tract, and kidney endothelial cells suggest a potentially higher risk in terms of SARS-CoV-2 invasion (7). Numerous case presentations or studies describe extrapulmonary manifestations such as vesicular and maculopapular mucosal lesions, ulcerations, and cutaneous manifestations (e.g. urticaria). In addition, opportunistic fungal infections due to dysbiosis, xerostomia due to decreased saliva production, and symptoms of gingivitis have been frequently noted in patients with COVID-19 (10, 11). The possibility of salivary glands being a reservoir for the SARS-CoV-2 virus has been suggested, since the salivary gland epithelium, compared to other tissues, has a significantly high level of ACE-2 expression, which was proved to be the functional receptor for cell entry. Furthermore, viable SARS-CoV-2 was isolated from the saliva before the appearance of lung lesions(12). Given the significance of saliva in viral transmission and the likelihood of salivary glands acting as a reservoir, the number of oral manifestations reported in our study was lesser than anticipated. Xerostomia, vesiculobullous lesions, aphtha-like lesions, dysgeusia, and anosmia were the most commonly reported oral symptoms in our study, regardless of gender.
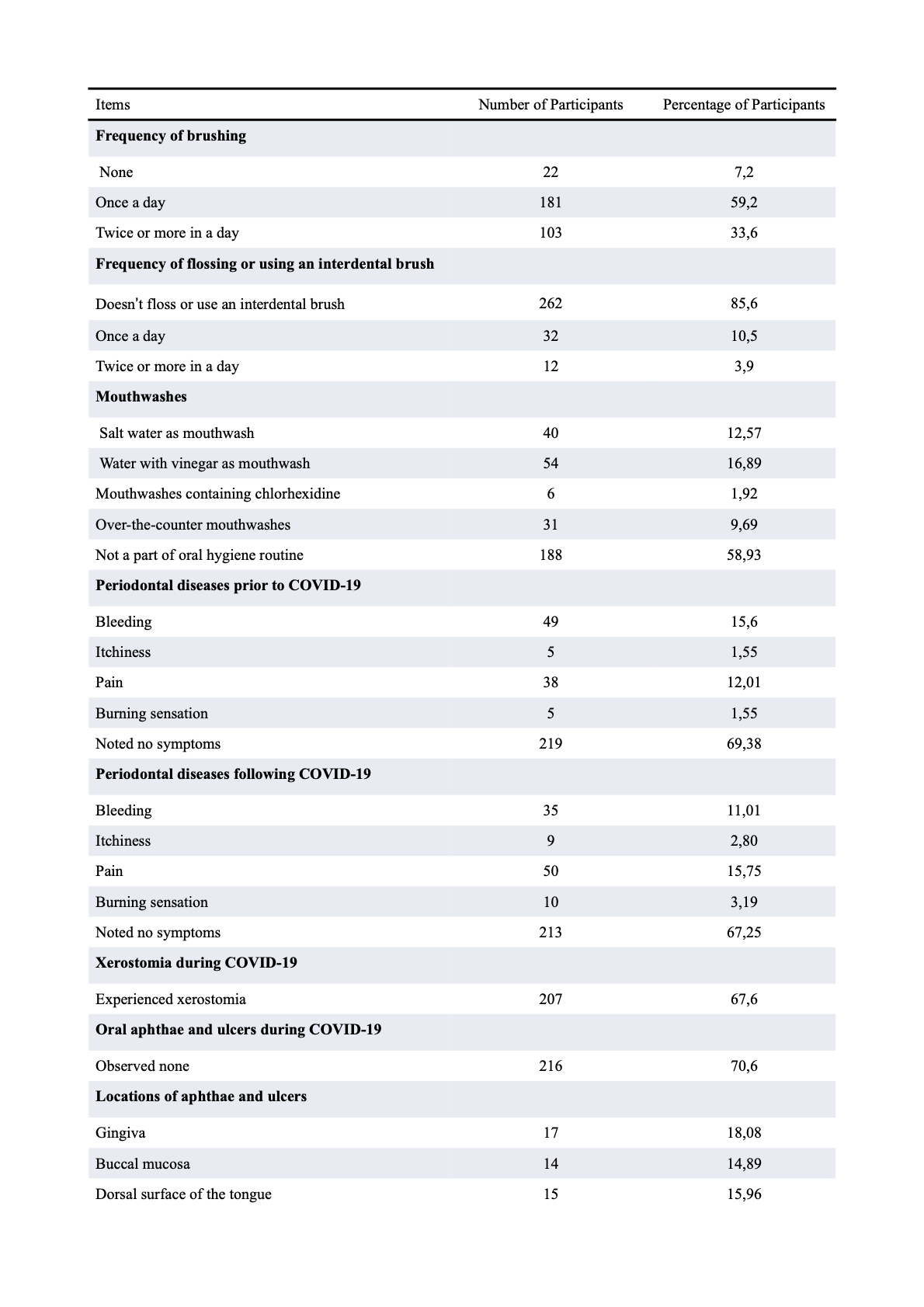
Xerostomia has been the most commonly reported finding in our study, with 67.6% of patients reporting it as a symptom during COVID-19. The fact that several case studies have identified respiratory tract infections as the primary cause of dry mouth supports the increase in xerostomia prevalence found in our study (13). Additionally, in a case series study of 108 COVID-19 patients with confirmed positive PCR tests in Wuhan, xerostomia was reported as a symptom in almost half of the patients (46%). In another study, xerostomia was reported in 16 patients, and only 1 patients’ complaint remained when the PCR tests turned negative. In a survey study with a sample of 573 patients, the symptom with the highest incidence, supporting our results, was xerostomia, which was seen in 47.6% of the patients(13).
In a cross-sectional study that included 500 patients, the two most common symptoms reported were found to be dysgeusia and xerostomia (28%), which were found in more than 50% of the patients (14). Maciel PP et al. also stated that there is a significant correlation between these two symptoms since the sense of taste is the main stimulus for saliva secretion, and that more than 50% of their COVID-19 patients listed both dry mouth and dysgeusia as a complaint during COVID-19(15).
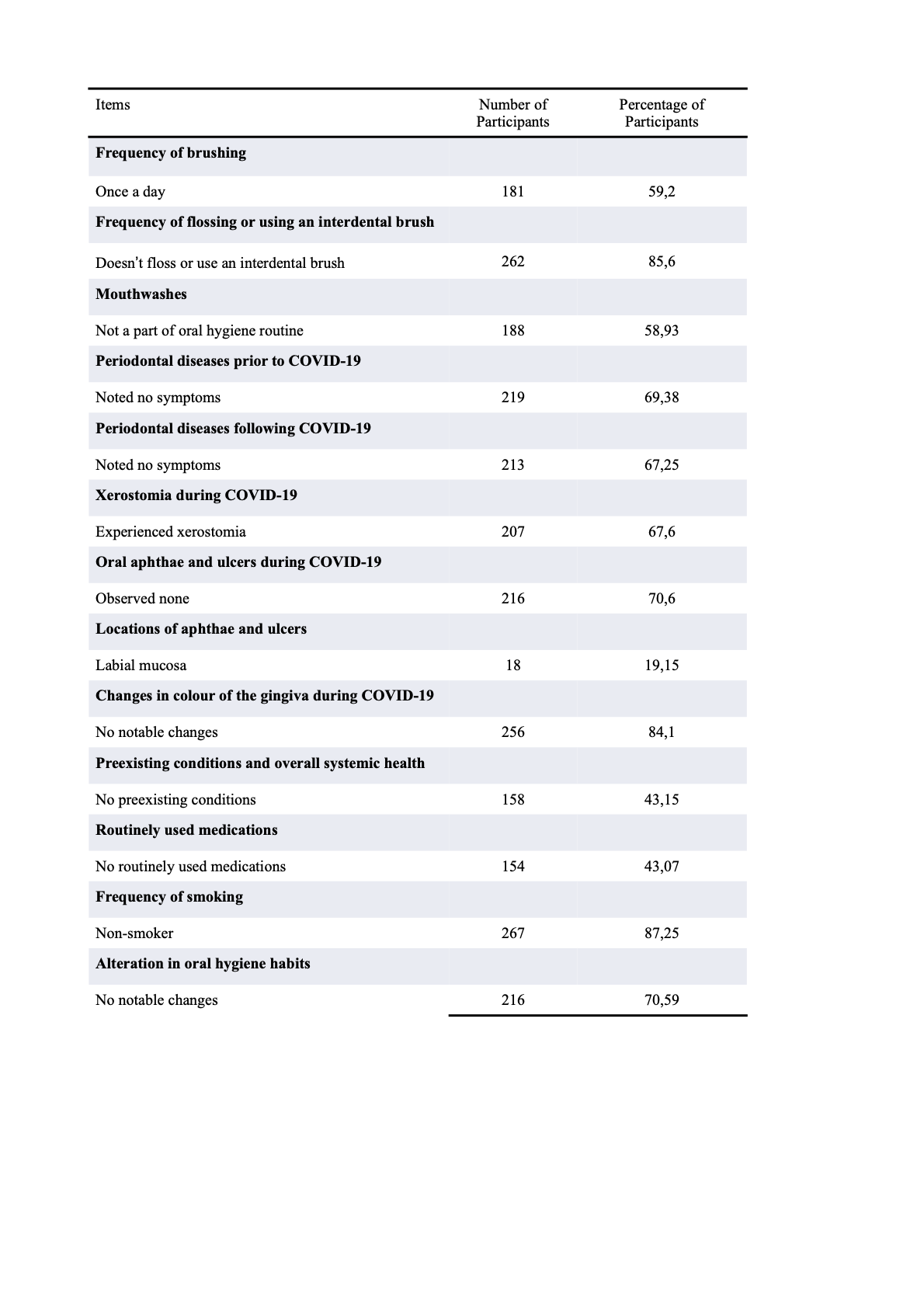
70.6% of the respondents stated that they did not have aphthous lesions and ulcers during COVID-19, the remaining participants that stated the opposite (29,4%) reported the labial mucosa (19.15%), followed by the gingival and palatal mucosa (18.08%), the dorsum of the tongue (15.96%), buccal mucosa (14.89%), ventral surface of the tongue and the floor of the mouth (13.84%) as sites. This percentage is in line with another survey-based study in which ulcerations were reported in 20.4% of participants (13).In a study on the oral pathogenesis of SARS-CoV-2, similar rates were reported in palatal and labial mucosal involvement with our study (26%, 22%, respectively) (7).In a case report presented by Carreras-Presas et al., aphthous lesions were detected in both keratinized and non-keratinized mucosa. Oral aphthae or ulcers were observed to appear in 29.4% of the volunteers, all of them being on the labial mucosa (10, 15). A clear relationship between COVID-19 and oral mucosal lesions has not yet been established. It is stated that many symptoms observed during the disease occur due to other viral, opportunistic, or secondary infections or due to the adverse effects of COVID-19 treatment, stress, and immunosuppression (16).In a case report by Rodríguez et al xerostomia was observed in 3 patients which was in line with our findings, however, the lesions and the burning sensation in the oral mucosa seen in 2 of the cases weren’t consistent with our results percentage-wise, although they were also reported in our study. In addition, all the reported cases reported in the study were mentioned to be immunocompromised, whereas, in our study, the aforementioned symptoms weren’t correlated to any degree of immunosuppression. Although oral lesions due to immunosuppression are known to develop more frequently, the evidence at hand has been lacking, researchers have been unable to establish a cause-and-effect relationship between coronavirus infection and oral lesions (17).
Oral health has a major impact on systemic health. Cytokines released in response to an oral infection triggering an inflammatory reaction in distant organs, aspiration of oral pathogens having a possibility to exacerbate an existing lung infection, and the mucosal surfaces of the airways becoming vulnerable to pathogen colonization by modification of salivary enzymes; reveals to us that there’s a correlation between oral hygiene and general health (18). Majority of the participants didn’t observe any changes in their oral hygiene habits during COVID-19 (70.5%) while 18.9% noted an increase, decrease in routine oral hygiene practices was reported the least (10.4%). The frequency of oral hygiene habits staying stagnant during COVID-19 was expected considering that majority of the participants’ practices were far from ideal even before the infection (59.2% of the participants brushed their teeth only once a day, 85.6% do not use dental floss or an interface brush). Likewise, 67.2% of the surveyees noted no inflammatory changes in the gingiva post-COVID-19, this indicates that oral hygiene habits can be preserved during the infection in spite of the symptoms. The decrease in the frequency of oral hygiene habits can be explained by the pain stemming from intraoral lesions or the patients’ mental state. In a literature review conducted by Bhujel et al. containing 12 studies, including case reports, review articles, and conference abstracts; necrotic gingivitis, desquamative gingivitis, hemorrhagic lesions/ulcers, and herpetic stomatitis have all been noted as soft tissue pathologies seen in COVID-19 patients. Lesions were most commonly seen on the tongue, followed by the palatal region, and lastly the buccal or labial mucosa (19). Our data suggest that COVID-19 can lead to a decrease in oral hygiene habits.
Every research has its limitations, ours included. The main limitation stems from the fact that this was a survey-based study, thus making it subjective. The participants' evaluation of oral symptoms based on their perceptions is not as objective as a clinicians’ systematic and scientific evaluation of a symptom aided by certain methods, available equipment, and resources. Analyzing the data this study procured, one still can’t conclusively determine whether the oral manifestations develop secondary to the side effects of COVID-19 treatment, are due to the deteriorated systemic health status and/or are caused/exacerbated by pre-existing chronic diseases. The severity of COVID-19 varies from case to case, as do the standards of oral hygiene, which can make pinpointing the main cause of intraoral lesions difficult. In order to reduce bias, new studies conducted with the elimination of patients with a history of oral symptoms or drugs and systemic conditions that may cause these symptoms are needed.
{kind=link}
{kind=link}
{kind=link}